

Burden of allergic respiratory disease: a systematic review
- PMID: 27708552
- PMCID: PMC5041537
- DOI: 10.1186/s12948-016-0049-9
Burden of allergic respiratory disease: a systematic review
Abstract
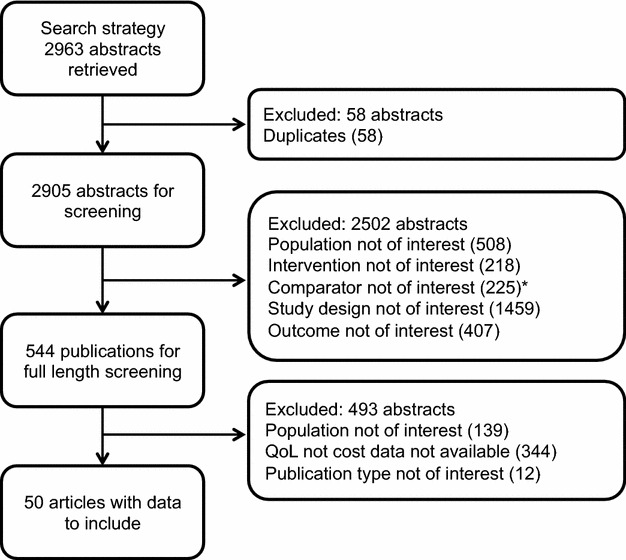
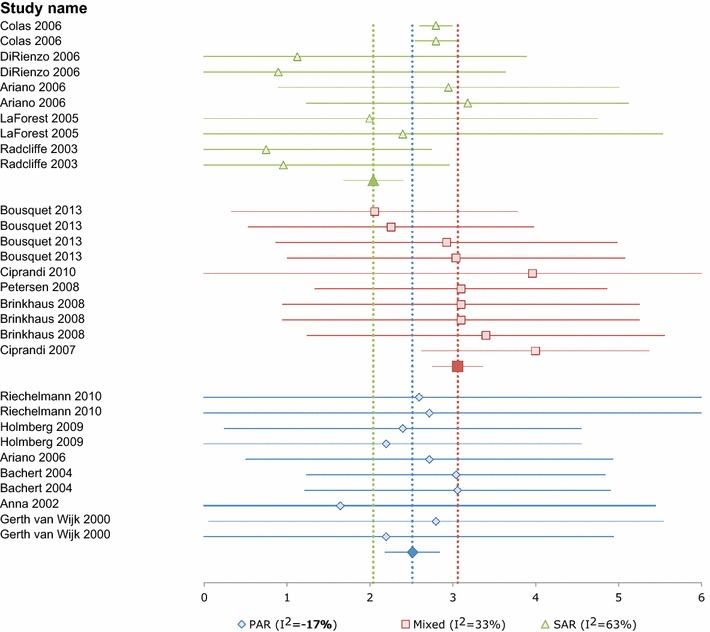
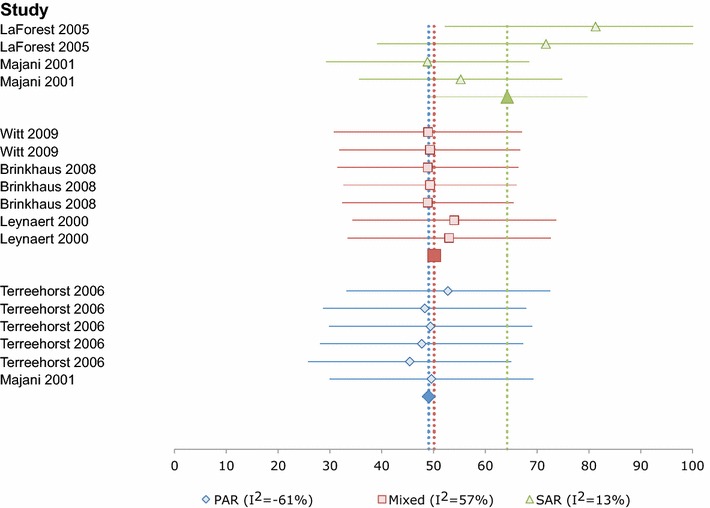
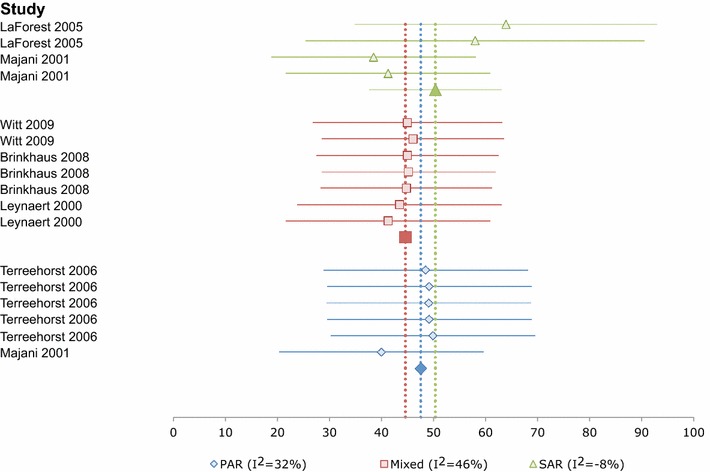
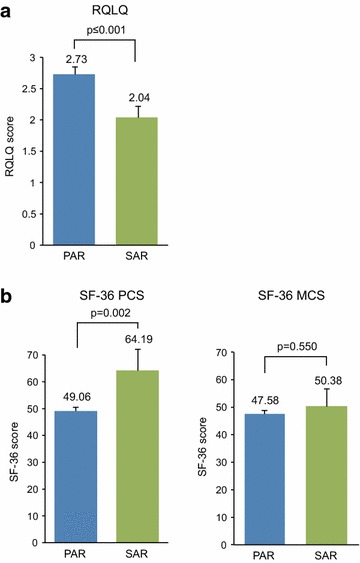
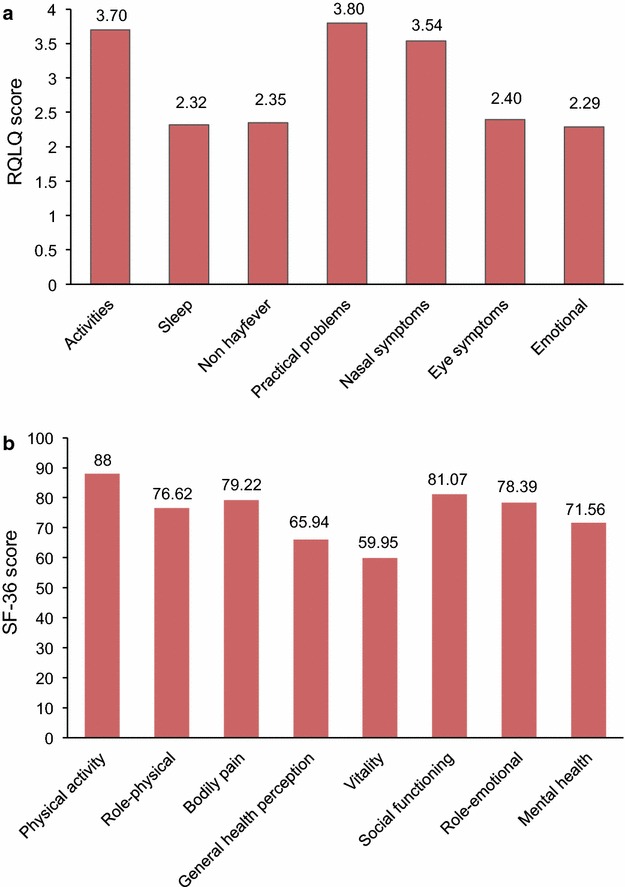
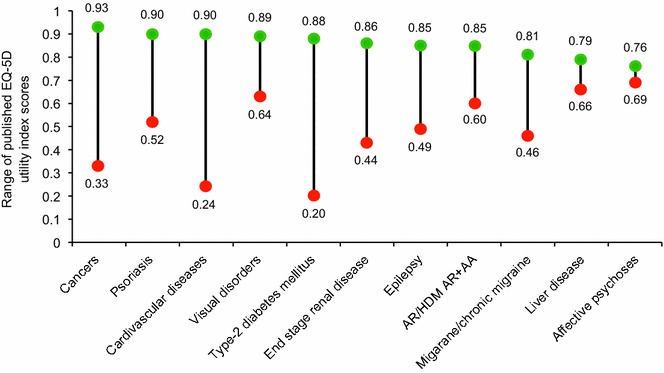
This meta-analysis compared the health-related quality of life (HRQL) of patients with allergic rhinitis (AR) and/or allergic asthma (AA) caused by perennial house dust mite (HDM) versus AR and/or AA caused by seasonal pollen allergy. Following a systematic search, the identified studies used the disease-specific rhinitis quality of life questionnaire or generic instruments (SF-36 and SF-12). Summary estimates obtained by meta-analysis showed that HRQL in patients with perennial HDM allergy was significantly worse than that of patients with seasonal pollen allergy, when measured by both disease-specific and generic HRQL instruments, and was reflected by an impact on both physical and mental health. A systematic review of cost data on AR and AA in selected European countries demonstrated that the majority of the economic burden was indirectly caused by high levels of absenteeism and presenteeism; there was little or no evidence of increasing or decreasing cost trends. Increased awareness of the detrimental effects of AR and/or AA on patients' HRQL and its considerable cost burden might encourage early diagnosis and treatment, in order to minimize the disease burden and ensure beneficial and cost-effective outcomes.
Keywords: Allergic asthma; Allergic rhinitis; Economic burden; Meta-analysis; Quality of life; Systematic review.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
