

doi: 10.1016/j.eats.2016.02.037.
eCollection 2016 Aug.
Distal Femoral Osteotomy: Lateral Opening Wedge Technique
Affiliations
- PMID: 27709028
- PMCID: PMC5039957
- DOI: 10.1016/j.eats.2016.02.037
Item in Clipboard
Distal Femoral Osteotomy: Lateral Opening Wedge Technique
Arthrosc Tech.
.
Abstract
Coronal limb malalignment is a significant contributor to asymmetric joint wear, gait abnormalities, and the development and progression of degenerative joint disease. Osteotomies about the knee were developed to realign the mechanical axis of the limb to unload the affected compartment. Valgus malalignment is less common than varus malalignment, but can contribute to a variety of clinical conditions, including lateral compartment cartilage defects and arthritis, lateral patellofemoral instability, and medial collateral ligament laxity. In this article, we describe our preferred operative technique for a lateral opening wedge varus-producing distal femoral osteotomy to correct mild to moderate valgus malalignment.
Figures
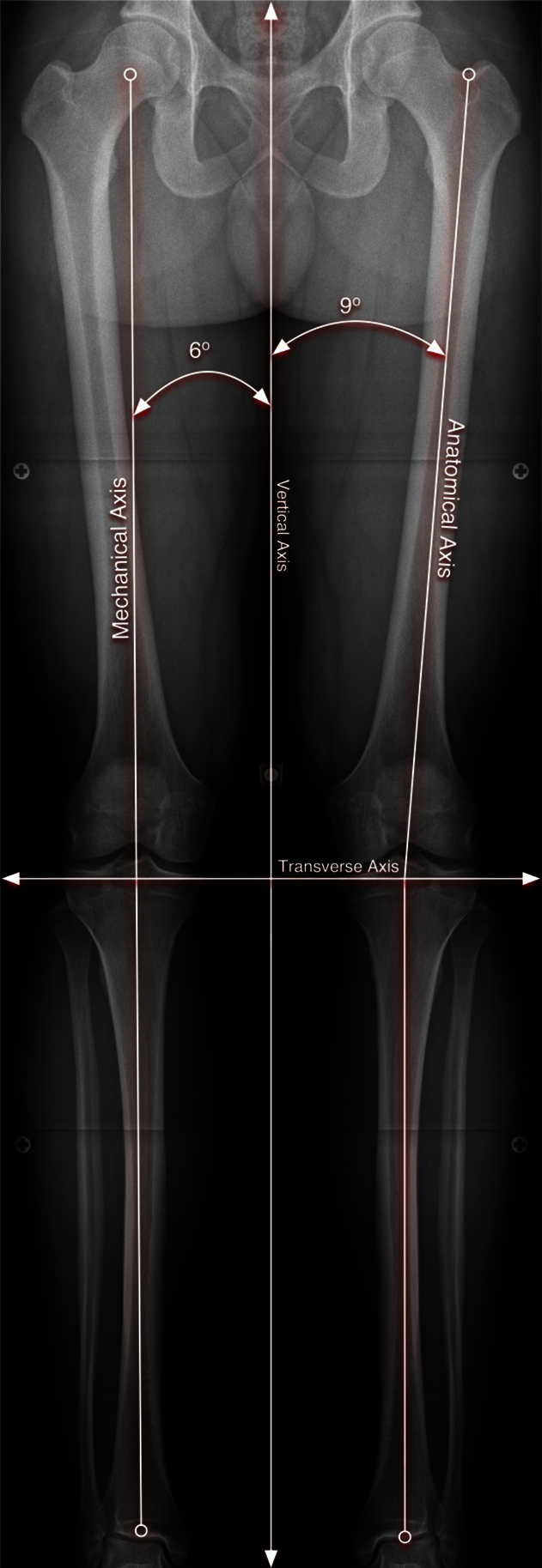
Depiction of both the normal mechanical and anatomic axis of the lower limb in a bilateral standing full-length anteroposterior radiograph. The mechanical axis follows a line from the femoral head through the center of the talus. The anatomic axis follows a line through the center of the femoral shaft through the center of the tibia to the center of the ankle.
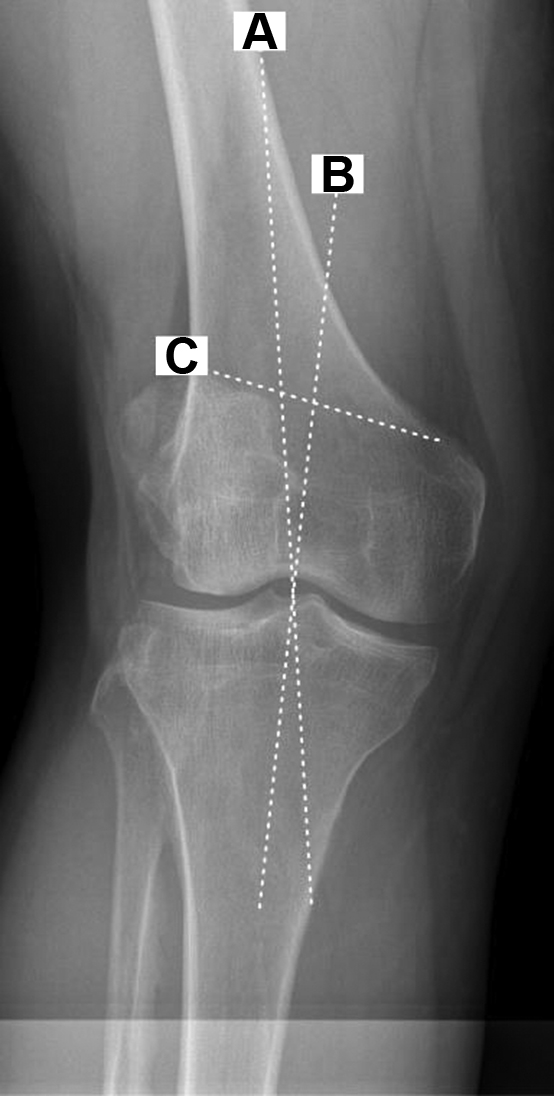
Calculation of the correction using the angle formed between the mechanical axis of the femur and tibia, respectively. This figure depicts a cropped view at the knee as a means to demonstrate how the deformity correction is determined. Lines drawn are as follows: Line A represents the desired mechanical axis of the limb from the center of the femoral head, passing through the center of the knee, which is the goal of correction in this case. Line B represents mechanical axis of the tibia passing from the center of the knee to the center of the tibiotalar joint at the ankle. In this case, the angle of correction measures 6 degrees. Line C represents the orientation at which the lateral opening wedge osteotomy will be made. Six degrees will be used to calculate the distance of opening required to achieve this correction.
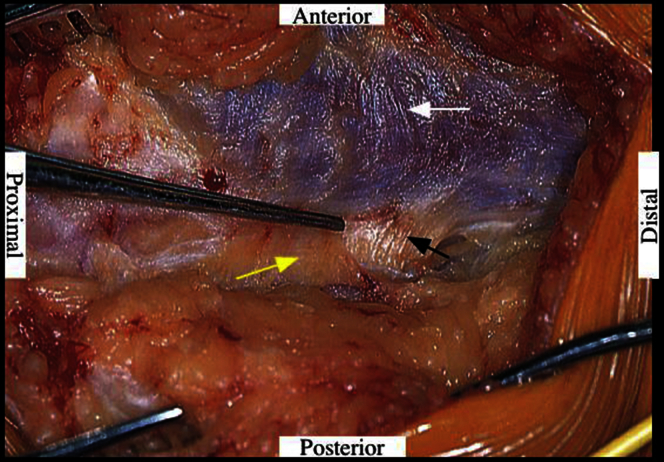
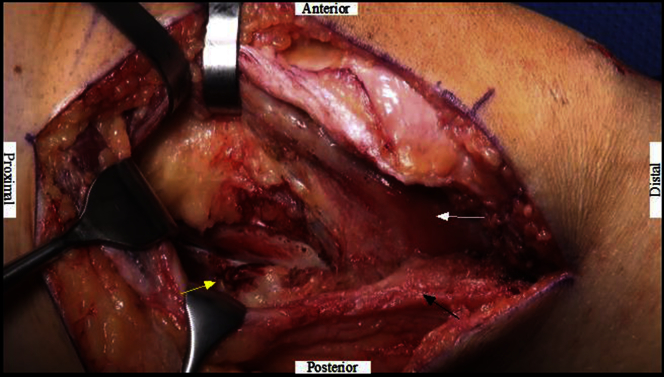
The intermuscular septum (white arrow) between vastus lateralis (black arrow) and biceps femoris, posterior aspect of vastus medialis (yellow arrow) is identified and elevated. Meticulous dissection in the correct plane is critical here as this will determine the exposure for the duration of the procedure.
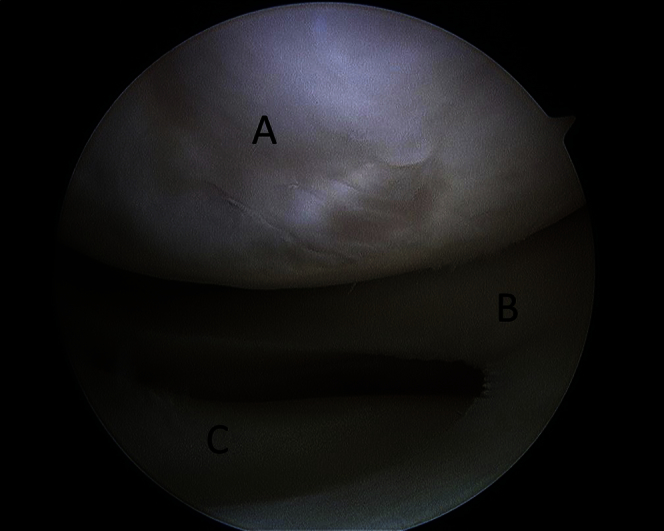
Depicted is an arthroscopic view of the lateral compartment of the knee from the anterolateral portal. Diagnostic arthroscopy can be used to assess for associated meniscoligamentous or cartilage injuries for concomitant procedures with the osteotomy. The denoted structures represent the lateral femoral condyle (A), the lateral meniscus (B), and the lateral tibial plateau (C).
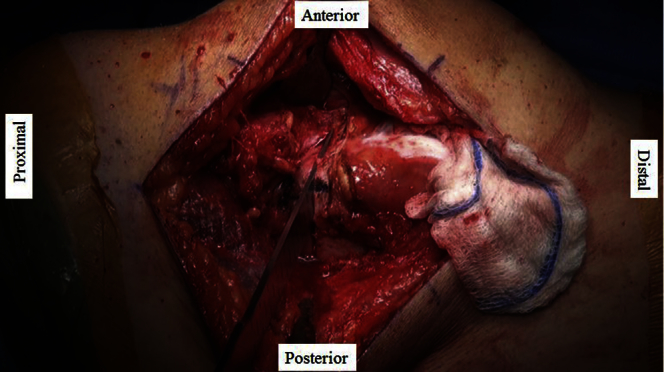
The vastus lateralis (white arrow) is carefully lifted up from intermuscular septum (black arrow) and the distal medial aspect of the femoral shaft is identified. Care is taken to coagulate arterial branches of profunda femoris (yellow arrow). This is an essential step in the exposure as significant bleeding can be encountered if not appropriately coagulated, which can cause significant complications to the limb, as well as affect visualization during the procedure.

Using fluoroscopic guidance, a guide pin is placed approximately 2 to 3 fingerbreadths proximal to the lateral epicondyle and aimed just proximal to the medial epicondyle. This will determine the angle of the osteotomy made first with the oscillating saw, and followed by osteotomes.
Osteotomes are used to complete the osteotomy in safe and effective manner. It is important not to violate the medial cortex during this step.

Intraoperative fluoroscopic imaging is used to confirm adequate correction and plate-screw construct on the lateral femoral cortex. Only after the mechanical axis has been corrected will the plate be placed and secured on the lateral femoral cortex.
References
-
- Brinkman J.M., Freiling D., Lobenhoffer P., Staubli A.E., van Heerwaarden R.J. Supracondylar femur osteotomies around the knee: Patient selection, planning, operative techniques, stability of fixation, and bone healing. Orthopade. 2014;43(Suppl 1):S1–S10. - PubMed
-
- Puddu G., Cipolla M., Cerullo G., Franco V., Gianni E. Osteotomies: The surgical treatment of the valgus knee. Sports Med Arthrosc. 2007;15:15–22. - PubMed
-
- Paccola C.A.J., Fogagnolo F. Open-wedge high tibial osteotomy: A technical trick to avoid loss of reduction of the opposite cortex. Knee Surg Sports Traumatol Arthrosc. 2005;13:19–22. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
