

Pharmacological properties of faster-acting insulin aspart vs insulin aspart in patients with type 1 diabetes receiving continuous subcutaneous insulin infusion: A randomized, double-blind, crossover trial
- PMID: 27709762
- PMCID: PMC5299522
- DOI: 10.1111/dom.12803
Pharmacological properties of faster-acting insulin aspart vs insulin aspart in patients with type 1 diabetes receiving continuous subcutaneous insulin infusion: A randomized, double-blind, crossover trial
Abstract
Aim: To evaluate the pharmacological characteristics of faster-acting insulin aspart (faster aspart) compared with insulin aspart (IAsp) during continuous subcutaneous insulin infusion (CSII).
Methods: In this randomized, double-blind, crossover trial, 48 men and women aged 18 to 64 years with type 1 diabetes mellitus (T1DM) received faster aspart and IAsp as a 0.15 U/kg bolus dose via CSII, on top of a basal rate (0.02 U/kg/h), in a glucose clamp setting (target 5.5 mmol/L).
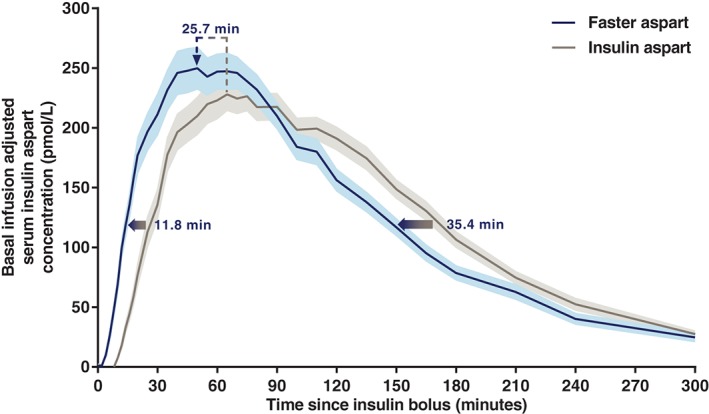
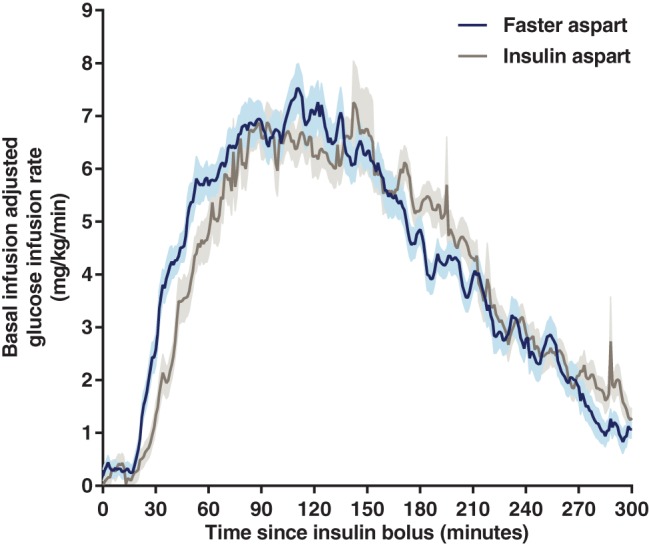
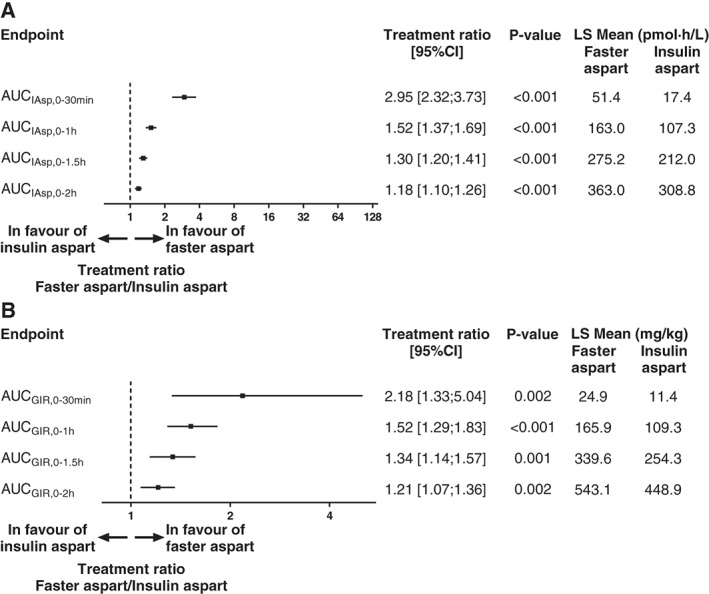
Results: After a CSII bolus dose, the pharmacokinetic/pharmacodynamic profiles for faster aspart were left-shifted compared with those for IAsp. For faster aspart vs IAsp, the early glucose-lowering effect (area under the curve for glucose infusion rate [GIR]0-30min ) was approximately 2-fold higher (least squares means 24.9 vs 11.4 mg/kg; estimated ratio faster aspart/IAsp 2.18, 95% confidence interval [CI] [1.33; 5.04]; P = .002), onset of glucose-lowering effect (time to early 50% of maximum GIR) occurred 11.1 minutes earlier (41.1 vs 52.3 minutes; 95% CI faster aspart - IAsp [-15.4; -6.9]; P<.001), and offset of glucose-lowering effect (time to late 50% of maximum GIR) occurred 24.0 minutes earlier (214.7 vs 238.7 minutes; 95% CI [-38.9; -9.1]; P=.002). Likewise, significantly greater early exposure and significantly earlier onset and offset of exposure were observed for faster aspart vs IAsp. Faster aspart and IAsp were both well tolerated.
Conclusions: In patients with T1DM using CSII, faster aspart better mimics the endogenous prandial insulin secretion and action than does IAsp. Faster aspart therefore has the potential to provide clinical benefits over current rapid-acting insulins in the insulin pump setting.
Keywords: insulin pump therapy; pharmacodynamics; pharmacokinetics; type 1 diabetes.
© 2016 The Authors. Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Figures
References
-
- Woerle HJ, Neumann C, Zschau S, et al. Impact of fasting and postprandial glycemia on overall glycemic control in type 2 diabetes. Importance of postprandial glycemia to achieve target HbA1c levels. Diabetes Res Clin Pract. 2007;77:280‐285. - PubMed
-
- Home PD. The pharmacokinetics and pharmacodynamics of rapid‐acting insulin analogues and their clinical consequences. Diabetes Obes Metab. 2012;14:780‐788. - PubMed
-
- Kalra S, Gupta Y. Ultra‐fast acting insulin analogues. Recent Pat Endocr Metab Immune Drug Discov. 2014;8:117‐123. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
