

Relapsing Polychondritis with Central Nervous System Involvement: Experience of Three Different Cases in a Single Center
- PMID: 27709866
- PMCID: PMC5056220
- DOI: 10.3346/jkms.2016.31.11.1846
Relapsing Polychondritis with Central Nervous System Involvement: Experience of Three Different Cases in a Single Center
Abstract
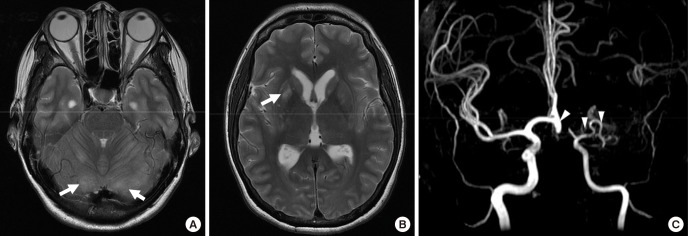
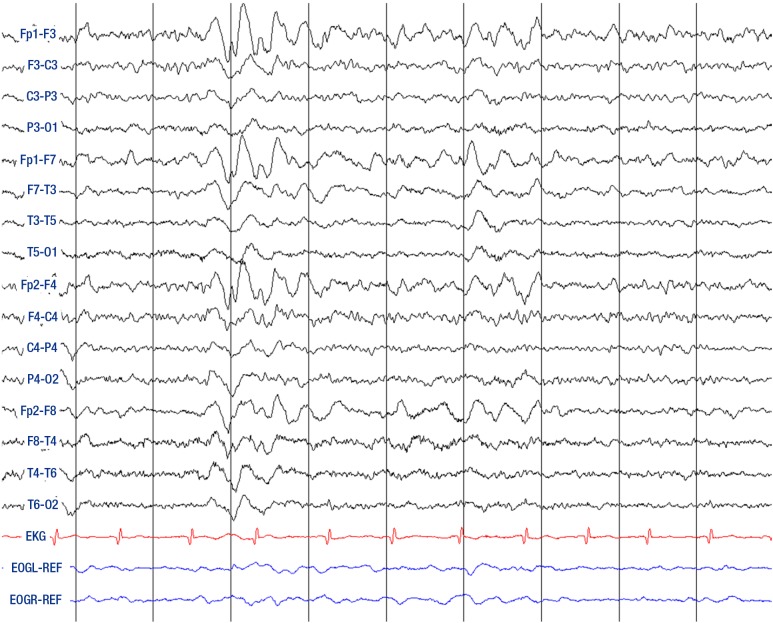
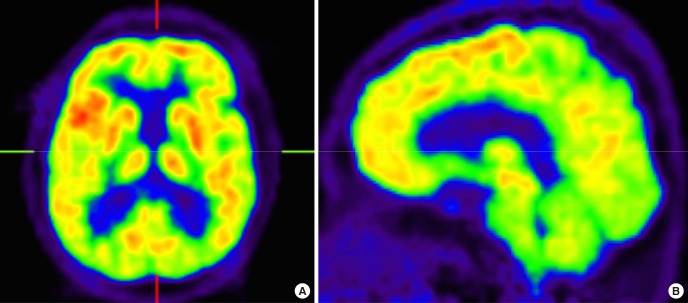
Relapsing polychondritis (RP) is an autoimmune disorder characterized by inflammation in cartilaginous structures including the ears, noses, peripheral joints, and tracheobronchial tree. It rarely involves the central nervous system (CNS) but diagnosis of CNS complication of RP is challenging because it can present with varying clinical features. Herein we report 3 cases of relapsing polychondritis involving CNS with distinct manifestations and clinical courses. The first patient presented with rhombencephalitis resulting in brain edema and death. The second patient had acute cognitive dysfunction due to limbic encephalitis. He was treated with steroid pulse therapy and recovered without sequelae. The third patient suffered aseptic meningitis that presented as dementia, which was refractory to steroid and immune suppressive agents. We also reviewed literature on CNS complications of RP.
Keywords: Dementia; Limbic Encephalitis; Meningoencephalitis; Relapsing Polychondritis.
Conflict of interest statement
The author has no potential conflicts of interest to disclose.
Figures
Comment in
-
Letter to the Editor: Central Nervous System Involvement in Relapsing Polychondritis, a Rare and Difficult Diagnosis: a Case Report.J Korean Med Sci. 2017 Jun;32(6):1048-1049. doi: 10.3346/jkms.2017.32.6.1048. J Korean Med Sci. 2017. PMID: 28480667 Free PMC article.
References
-
- McAdam LP, O’Hanlan MA, Bluestone R, Pearson CM. Relapsing polychondritis: prospective study of 23 patients and a review of the literature. Medicine (Baltimore) 1976;55:193–215. - PubMed
-
- Puéchal X, Terrier B, Mouthon L, Costedoat-Chalumeau N, Guillevin L, Le Jeunne C. Relapsing polychondritis. Joint Bone Spine. 2014;81:118–124. - PubMed
-
- Sampaio L, Silva L, Mariz E, Ventura F. Central nervous system involvement in relapsing polychondritis. Joint Bone Spine. 2010;77:619–620. - PubMed
-
- Kashihara K, Kawada S, Takahashi Y. Autoantibodies to glutamate receptor GluRepsilon2 in a patient with limbic encephalitis associated with relapsing polychondritis. J Neurol Sci. 2009;287:275–277. - PubMed
-
- Mihara T, Ueda A, Hirayama M, Takeuchi T, Yoshida S, Naito K, Yamamoto H, Mutoh T. Detection of new anti-neutral glycosphingolipids antibodies and their effects on Trk neurotrophin receptors. FEBS Lett. 2006;580:4991–4995. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
