

Bioprinting 3D microfibrous scaffolds for engineering endothelialized myocardium and heart-on-a-chip
- PMID: 27710832
- PMCID: PMC5198581
- DOI: 10.1016/j.biomaterials.2016.09.003
Bioprinting 3D microfibrous scaffolds for engineering endothelialized myocardium and heart-on-a-chip
Erratum in
-
Corrigendum to 'Bioprinting 3D microfibrous scaffolds for engineering cardiac tissues and heart-on-a-chip' [Biomaterials Volume 110, (2016) Pages 45-59].Biomaterials. 2025 Nov;322:123363. doi: 10.1016/j.biomaterials.2025.123363. Epub 2025 May 10. Biomaterials. 2025. PMID: 40348645 No abstract available.
Abstract
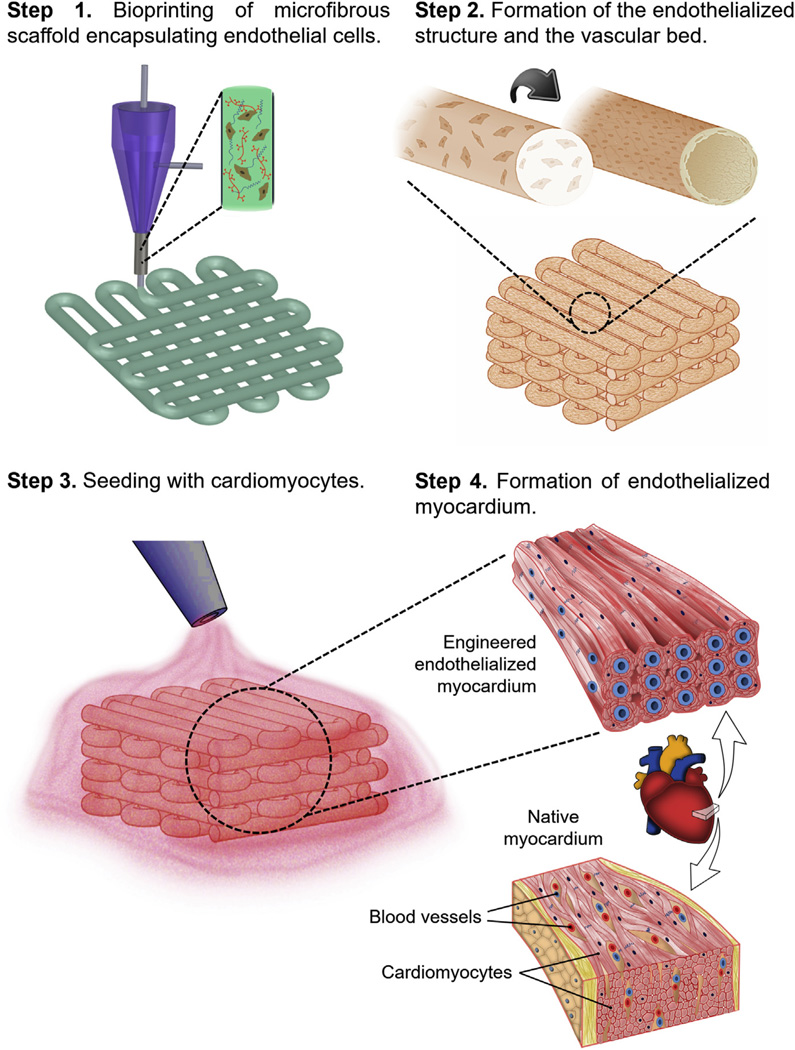
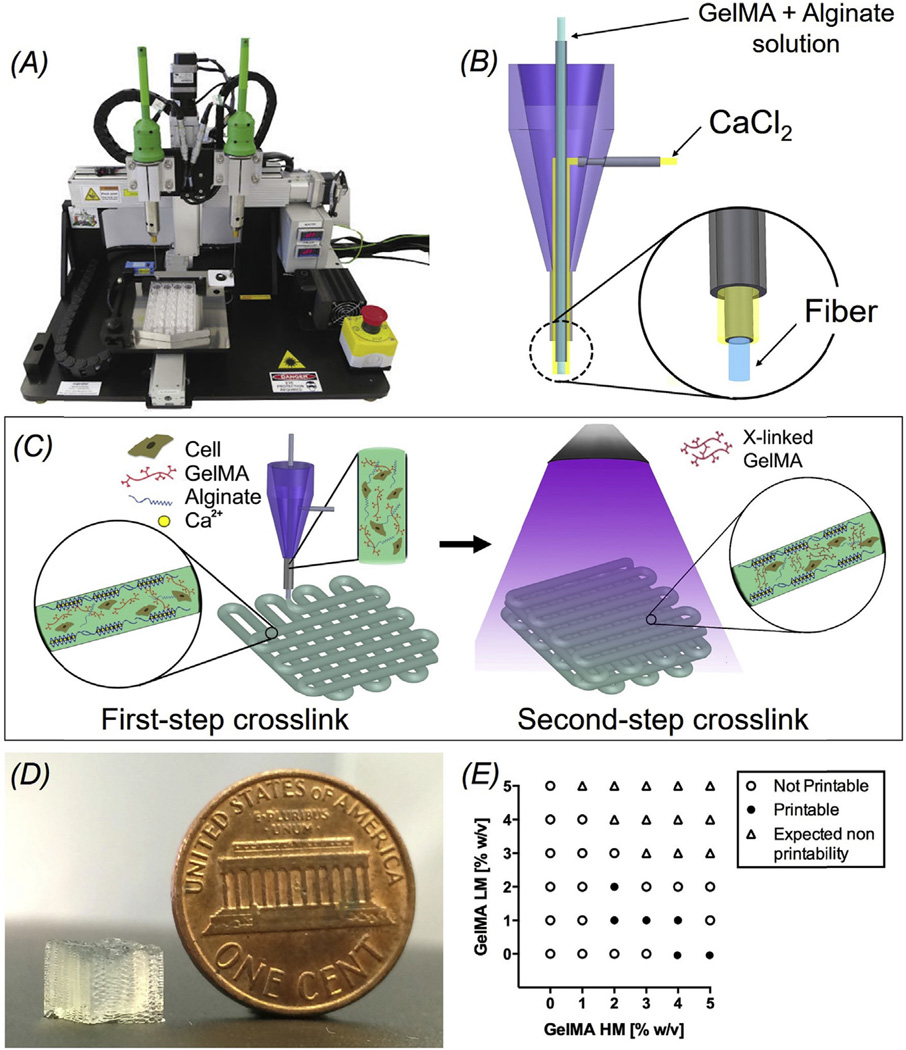
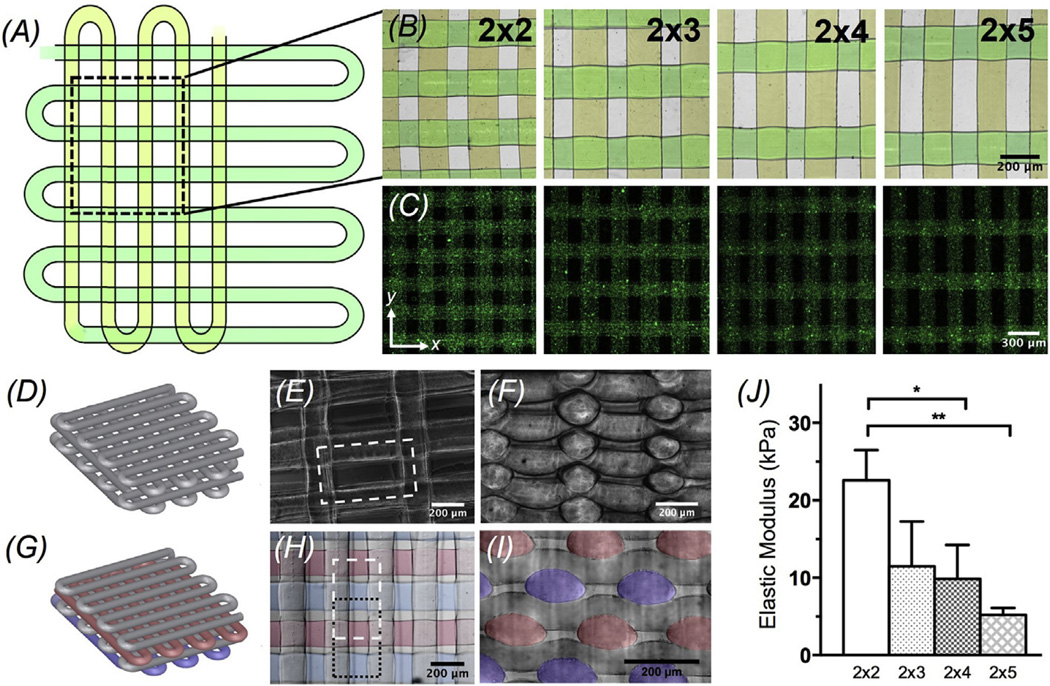
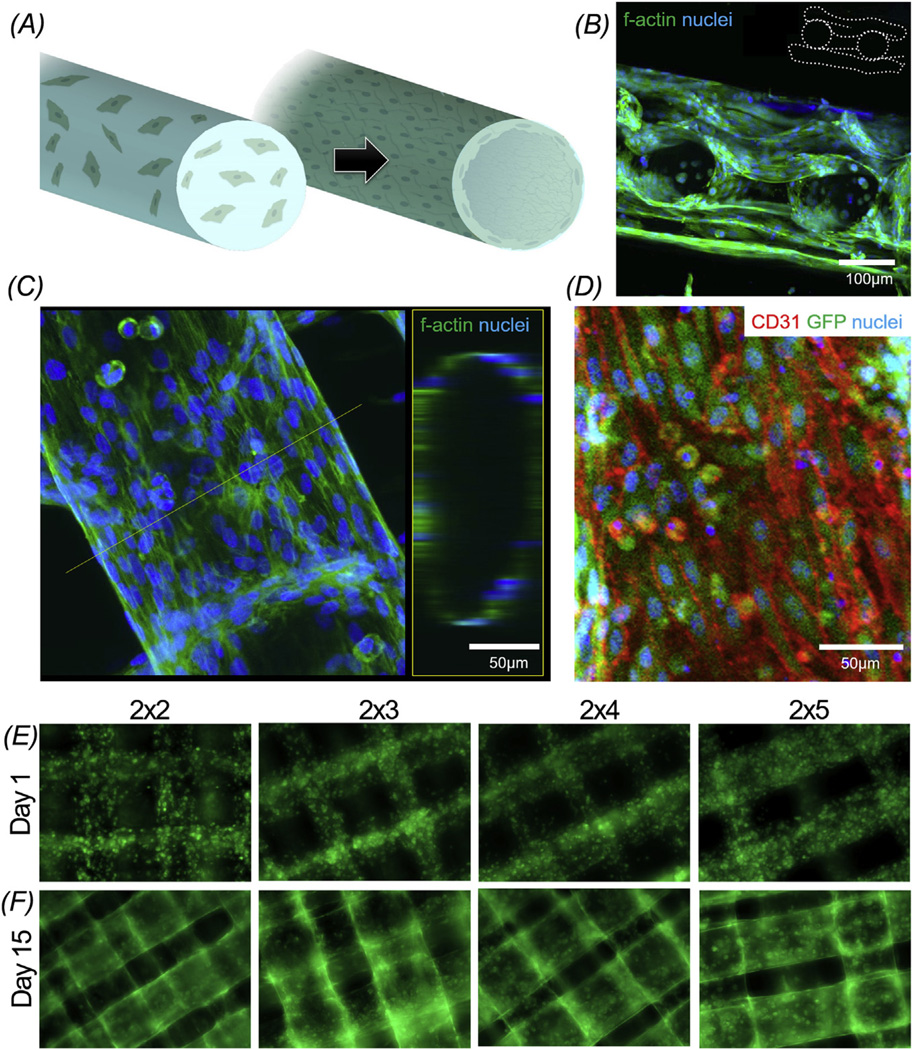
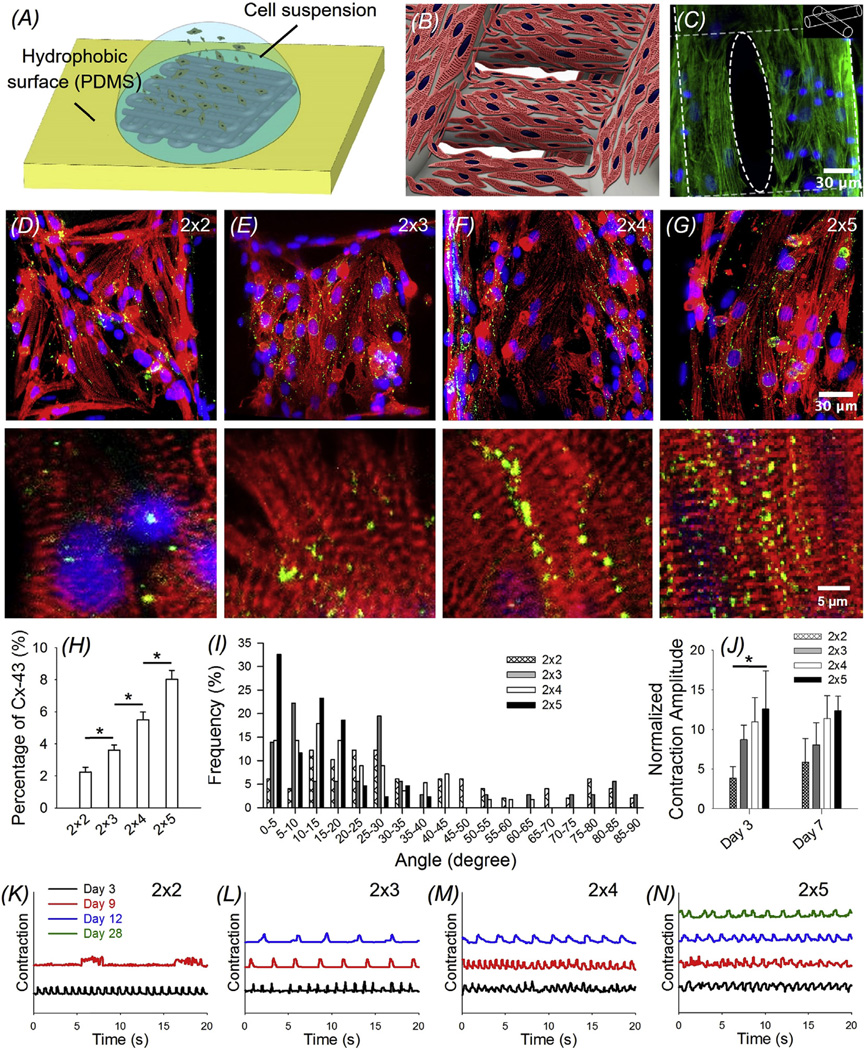
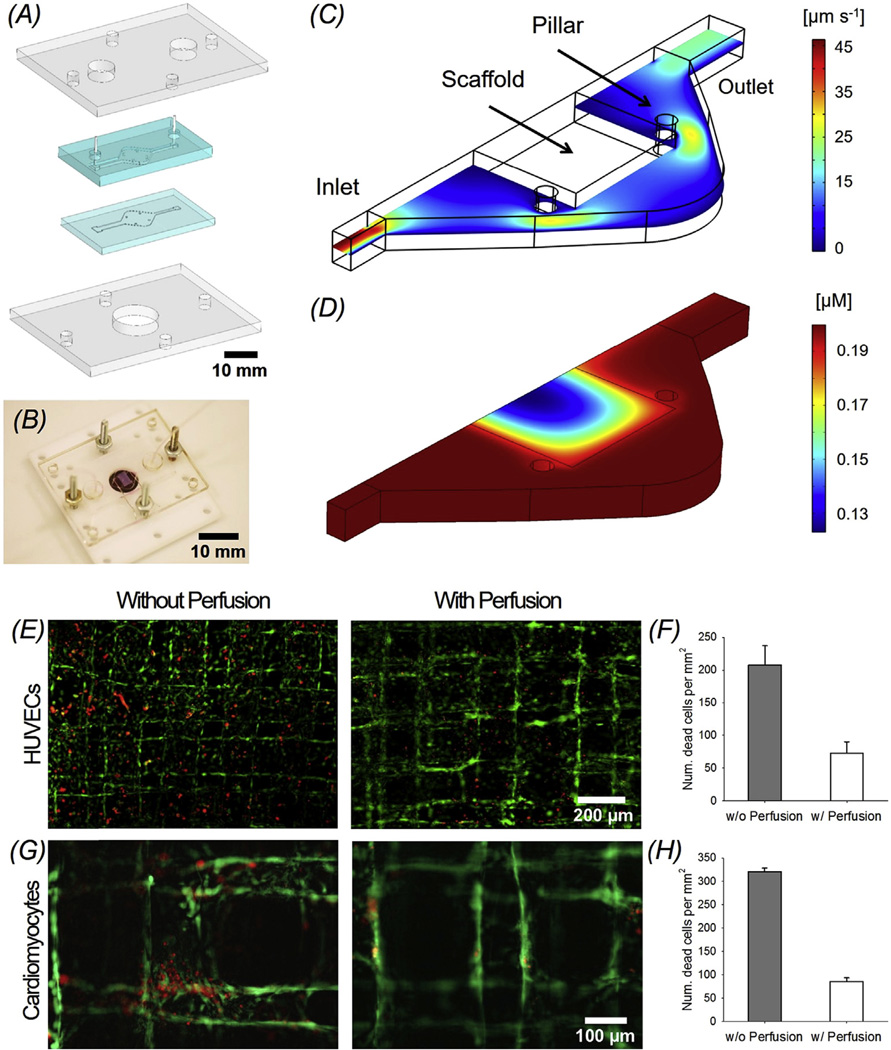
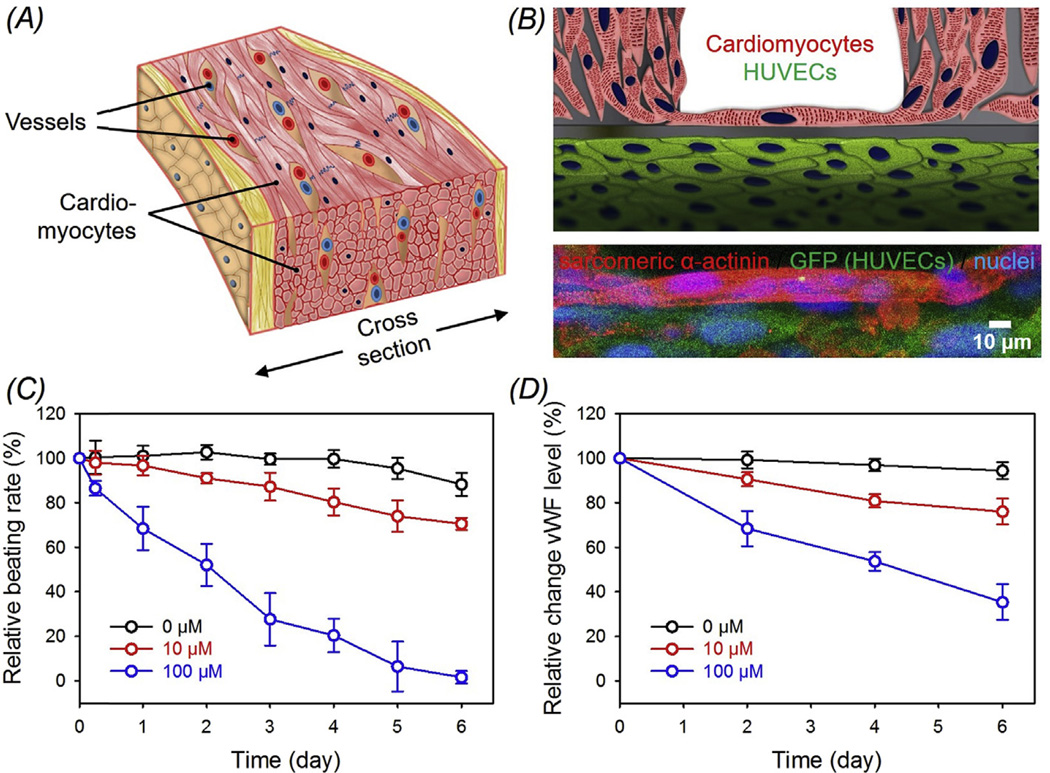
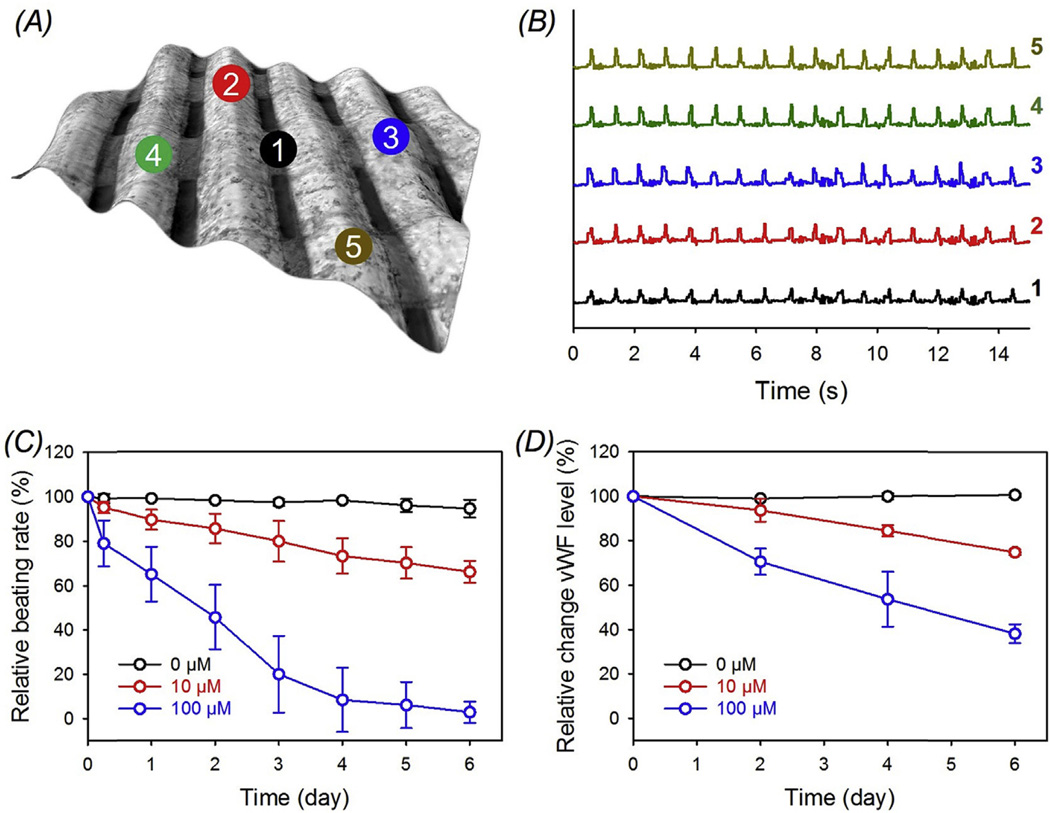
Engineering cardiac tissues and organ models remains a great challenge due to the hierarchical structure of the native myocardium. The need of integrating blood vessels brings additional complexity, limiting the available approaches that are suitable to produce integrated cardiovascular organoids. In this work we propose a novel hybrid strategy based on 3D bioprinting, to fabricate endothelialized myocardium. Enabled by the use of our composite bioink, endothelial cells directly bioprinted within microfibrous hydrogel scaffolds gradually migrated towards the peripheries of the microfibers to form a layer of confluent endothelium. Together with controlled anisotropy, this 3D endothelial bed was then seeded with cardiomyocytes to generate aligned myocardium capable of spontaneous and synchronous contraction. We further embedded the organoids into a specially designed microfluidic perfusion bioreactor to complete the endothelialized-myocardium-on-a-chip platform for cardiovascular toxicity evaluation. Finally, we demonstrated that such a technique could be translated to human cardiomyocytes derived from induced pluripotent stem cells to construct endothelialized human myocardium. We believe that our method for generation of endothelialized organoids fabricated through an innovative 3D bioprinting technology may find widespread applications in regenerative medicine, drug screening, and potentially disease modeling.
Keywords: Bioprinting; Cardiac tissue engineering; Cardiovascular toxicity; Heart-on-a-chip; Vascularization.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Figures
References
-
- Chiu L, Iyer RK, Reis LA, Nunes SS, Radisic M. Cardiac tissue engineering: current state and perspectives. Front. Biosci. 2011;17:1533–1550. - PubMed
-
- Chiu LL, Radisic M. Cardiac tissue engineering. Curr. Opin. Chem. Eng. 2013;2:41–52.
-
- Zhang YS, Khademhosseini A. Seeking the Right context for evaluating nanomedicine: from tissue models in petri dishes to microfluidic organs-on-a-chip. Nanomedicine. 2015;10:685–688. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
