

Resources Required for Cervical Cancer Prevention in Low- and Middle-Income Countries
- PMID: 27711124
- PMCID: PMC5053484
- DOI: 10.1371/journal.pone.0164000
Resources Required for Cervical Cancer Prevention in Low- and Middle-Income Countries
Abstract
Background: Cervical cancer is the fourth leading cause of cancer death in women, with 85% of cases and deaths occurring in developing countries. While organized screening programs have reduced cervical cancer incidence in high-income countries through detection and treatment of precancerous lesions, the implementation of organized screening has not been effective in low-resource settings due to lack of infrastructure and limited budgets. Our objective was to estimate the cost of comprehensive primary and secondary cervical cancer prevention in low- and middle-income countries.
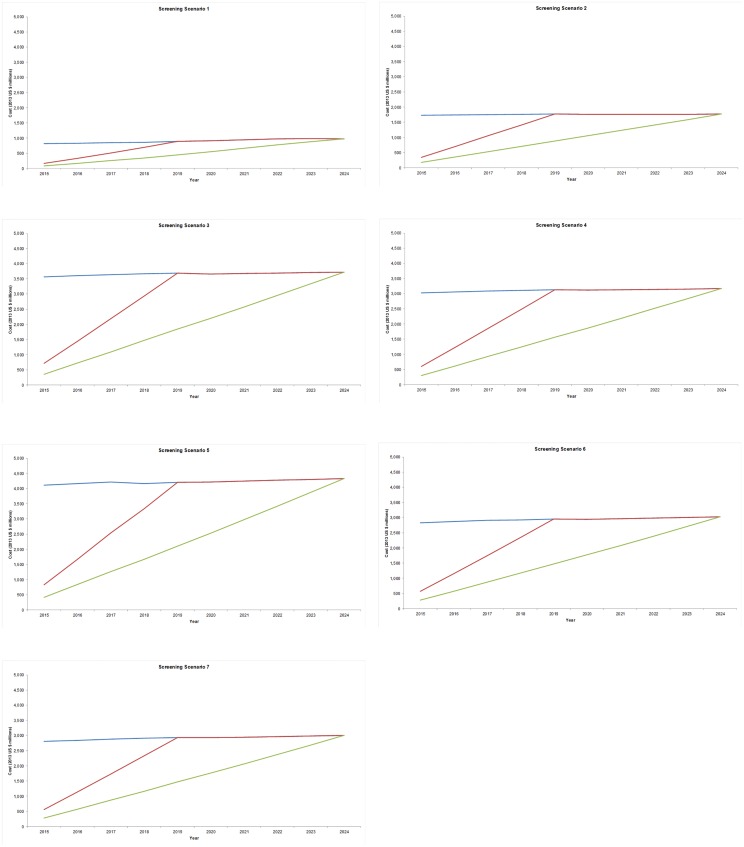
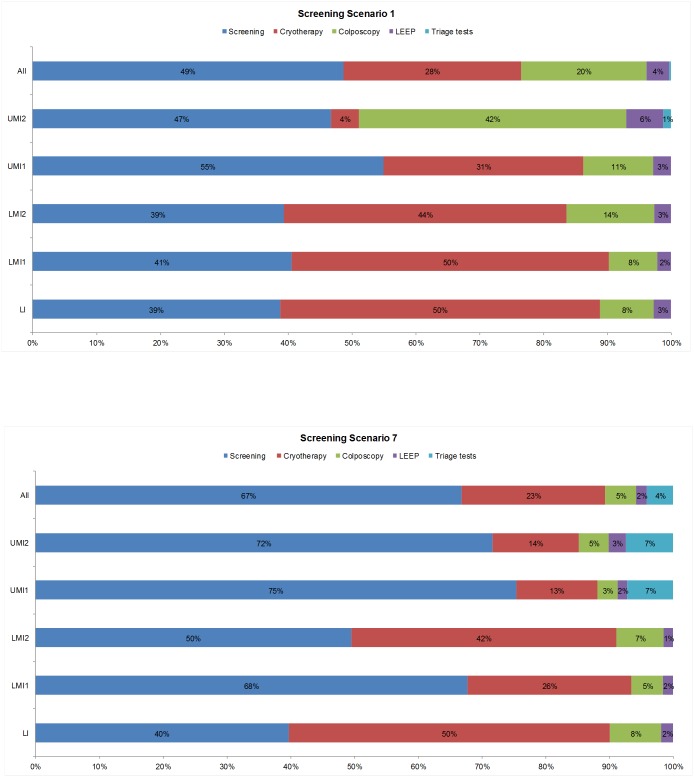
Methods and findings: We performed a modeling analysis to estimate 1) for girls aged 10 years, the cost of 2-dose human papillomavirus (HPV) vaccination; and 2) for women aged 30 to 49 years, the cost of cervical cancer screening (with visual inspection with acetic acid (VIA), HPV testing, or cytology) and preventive treatment in 102 low- and middle-income countries from 2015 to 2024. We used an Excel-based costing and service utilization model to estimate financial costs (2013 US$) based on prevalence of HPV, prevalence of precancerous lesions, and screening test performance. Where epidemiologic data were unavailable, we extrapolated from settings with data using an individual-based microsimulation model of cervical carcinogenesis (calibrated to 20 settings) and multivariate regression. Total HPV vaccination costs ranged from US$8.6 billion to US$24.2 billion for all scenarios considered (immediate, 5-year, or 10-year roll-out; price per dose US$4.55-US$70 by country income level). The total cost of screening and preventive treatment ranged from US$5.1 billion (10-year roll-out, screening once at age 35 years) to US$42.3 billion (immediate roll-out, high intensity screening). Limitations of this analysis include the assumption of standardized protocols by country income level that did not account for the potential presence of multiple screening modalities or management strategies within a country, and extrapolation of cost and epidemiologic data to settings where data were limited.
Conclusions: The estimated cost of comprehensive cervical cancer prevention with 2-dose HPV vaccination of 10-year-old girls and screening of women aged 30 to 49 years ranges from US$13.7 billion to US$66.5 billion, depending on speed of roll-out, vaccine price per dose, and screening test and frequency. Findings demonstrate the substantial impact of vaccine price in middle-income countries that are not eligible for assistance from Gavi, the Vaccine Alliance. Replacing routine cytology with HPV-based screening may reduce total costs. Data on the health impact and relative cost-effectiveness of strategies are needed to determine the best value for public health dollars.
Conflict of interest statement
NGC, MS, AC, JJK, and SCR declare support from the American Cancer Society for the submitted work. Inputs to the CERVIVAC model are described in the main text and Supporting Information. The CERVIVAC model was developed in collaboration with the Pan American Health Organization ProVac Initiative, and inquiries regarding the model can be made through ProVac. Cost projections for individual countries are not available, but rather are aggregated by region or income tier as documented in the text. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C, et al. (2013) GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11 [Internet]. Lyon, France: International Agency for Research on Cancer.
-
- Gavi, The Vaccine Alliance. Human papillomavirus vaccine support: Record low price agreed for HPV vaccines. Available at: http://www.gavi.org/support/nvs/human-papillomavirus/.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
