

Anorectal and Pelvic Pain
- PMID: 27712641
- PMCID: PMC5123821
- DOI: 10.1016/j.mayocp.2016.08.011
Anorectal and Pelvic Pain
Abstract
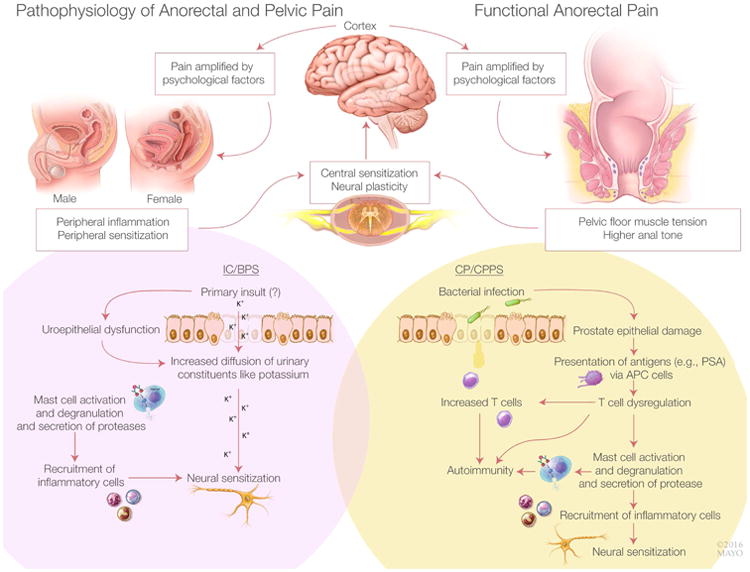
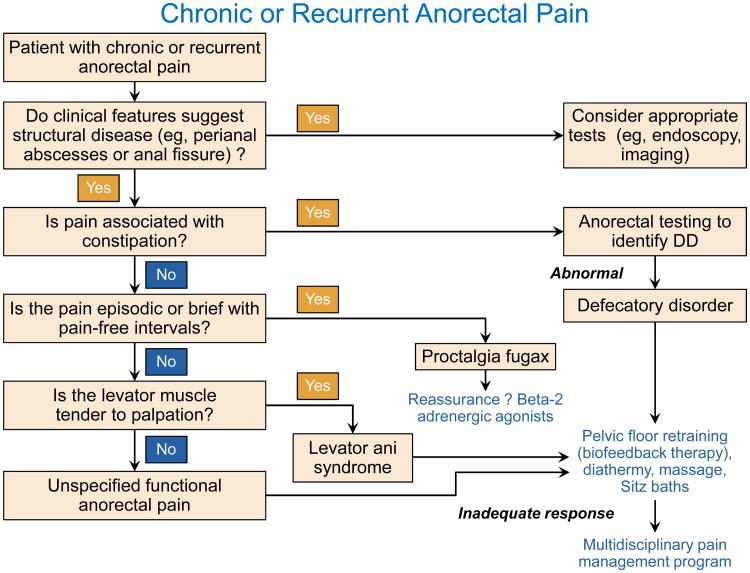
Although pelvic pain is a symptom of several structural anorectal and pelvic disorders (eg, anal fissure, endometriosis, and pelvic inflammatory disease), this comprehensive review will focus on the 3 most common nonstructural, or functional, disorders associated with pelvic pain: functional anorectal pain (ie, levator ani syndrome, unspecified anorectal pain, and proctalgia fugax), interstitial cystitis/bladder pain syndrome, and chronic prostatitis/chronic pelvic pain syndrome. The first 2 conditions occur in both sexes, while the latter occurs only in men. They are defined by symptoms, supplemented with levator tenderness (levator ani syndrome) and bladder mucosal inflammation (interstitial cystitis). Although distinct, these conditions share several similarities, including associations with dysfunctional voiding or defecation, comorbid conditions (eg, fibromyalgia, depression), impaired quality of life, and increased health care utilization. Several factors, including pelvic floor muscle tension, peripheral inflammation, peripheral and central sensitization, and psychosocial factors, have been implicated in the pathogenesis. The management is tailored to symptoms, is partly supported by clinical trials, and includes multidisciplinary approaches such as lifestyle modifications and pharmacological, behavioral, and physical therapy. Opioids should be avoided, and surgical treatment has a limited role, primarily in refractory interstitial cystitis.
Copyright © 2016 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Dr. Bharucha reports personal fees from Allergan Inc, personal fees from Johnson and Johnson Inc, personal fees and other from Medspira, personal fees from Ironwood Pharma, personal fees from GI Care Pharma, personal fees from National Center for Pelvic Pain Research, personal fees from Salix, personal fees from Macmillan Medical Communications, personal fees from Forum Pharmaceuticals, outside the submitted work; In addition, Dr. Bharucha has patented an Anorectal manometry device with royalties paid to Medspira, Inc., and has a pending patent Anorectal manometry probe fixation device licensed to Medtronic, Inc. Dr. Lee has nothing to disclose.
Figures
References
-
- Clemens JQ. Male and female pelvic pain disorders - is it all in their heads? J Urol. 2008;179:813–814. - PubMed
-
- Potts JM, Payne CK. Urologic chronic pelvic pain. Pain. 2012;153(4):755–758. - PubMed
-
- Hanno PM, Erickson D, Moldwin R, Faraday MM. Diagnosis and treatment of interstitial cystitis/bladder pain syndrome: AUA guideline amendment. J Urol. 2015;193(5):1545–1553. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
