

Microtia Reconstruction
- PMID: 27712823
- PMCID: PMC5950715
- DOI: 10.1016/j.fsc.2016.06.011
Microtia Reconstruction
Abstract
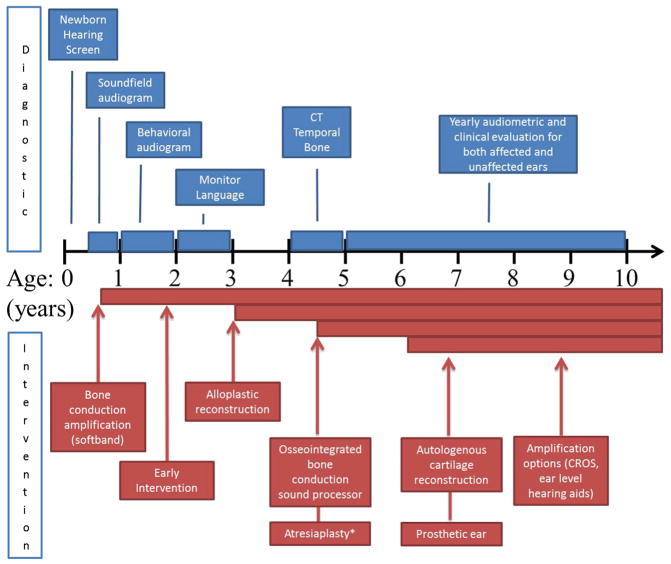
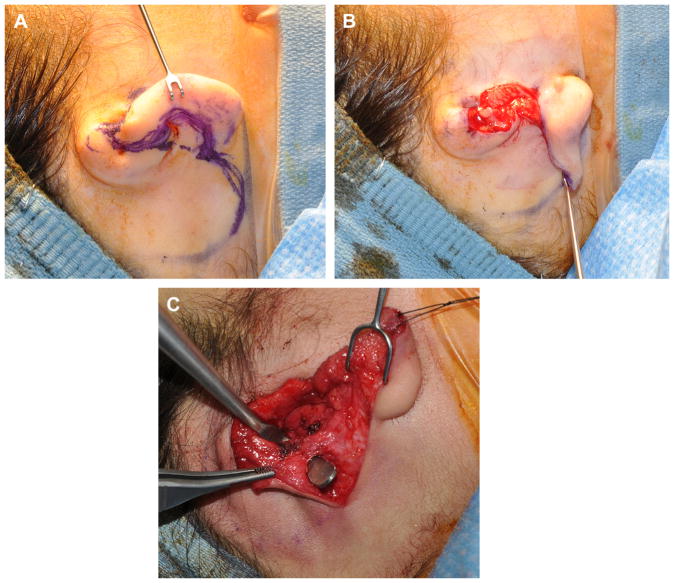
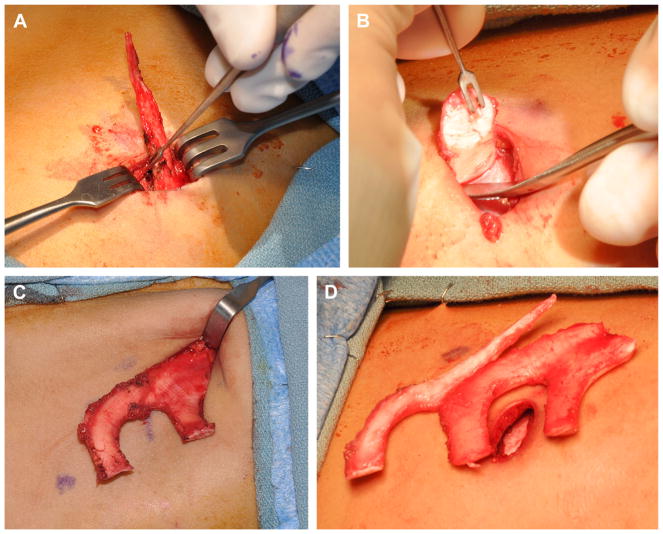
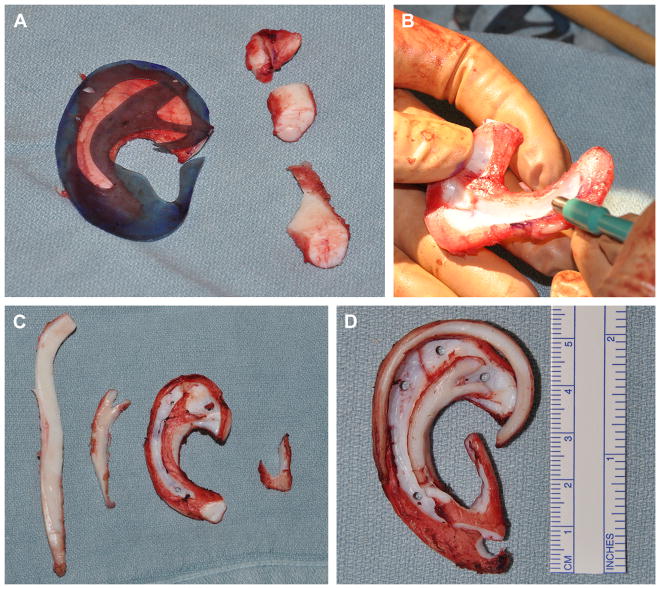
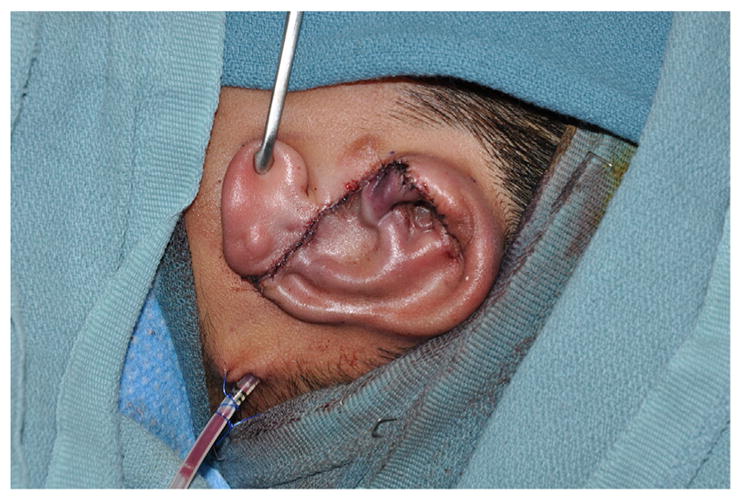
Microtia reconstruction is a challenging endeavor that has seen significant technique evolution. It is important to educate patients and their families to determine the best hearing rehabilitation and ear reconstructive options. Microtia is often associated with aural atresia, hearing loss, and craniofacial syndromes. Optimal care is provided by multiple disciplines, including a reconstructive surgeon, an otologic surgeon, an audiologist, and a craniofacial pediatrician. Microtia management includes observation, prosthetic ear, autologous cartilage reconstruction, or alloplastic implant placement. Hearing management options are observation, bone conduction sound processor, or atresiaplasty with and without hearing aids. Appropriate counseling should be done to manage expectations.
Keywords: Alloplastic reconstruction; Auricular reconstruction; Autologous reconstruction; Cartilage graft; Microtia; Microtia management.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures







References
-
- Castilla EE, Orioli IM. Prevalence rates of microtia in South America. Int J Epidemiol. 1986;15:364–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
