

Use of explicit ICD9-CM codes to identify adult severe sepsis: impacts on epidemiological estimates
- PMID: 27716355
- PMCID: PMC5047045
- DOI: 10.1186/s13054-016-1497-9
Use of explicit ICD9-CM codes to identify adult severe sepsis: impacts on epidemiological estimates
Abstract
Background: Severe sepsis is a challenge for healthcare systems, and epidemiological studies are essential to assess its burden and trends. However, there is no consensus on which coding strategy should be used to reliably identify severe sepsis. This study assesses the use of explicit codes to define severe sepsis and the impacts of this on the incidence and in-hospital mortality rates.
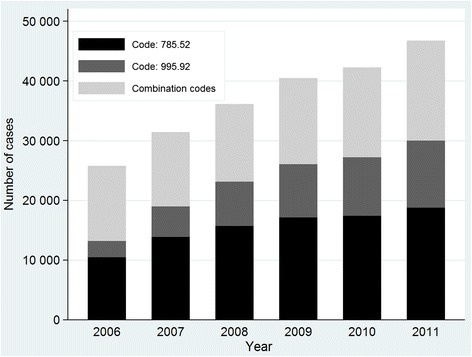
Methods: We examined episodes of severe sepsis in adults aged ≥18 years registered in the 2006-2011 national hospital discharge database, identified in an exclusive manner by two ICD-9-CM coding strategies: (1) those assigned explicit ICD-9-CM codes (995.92, 785.52); and (2) those assigned combined ICD-9-CM infection and organ dysfunction codes according to modified Martin criteria. The coding strategies were compared in terms of the populations they defined and their relative implementation. Trends were assessed using Joinpoint regression models and expressed as annual percentage change (APC).
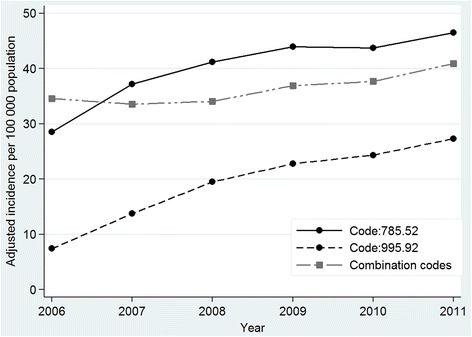
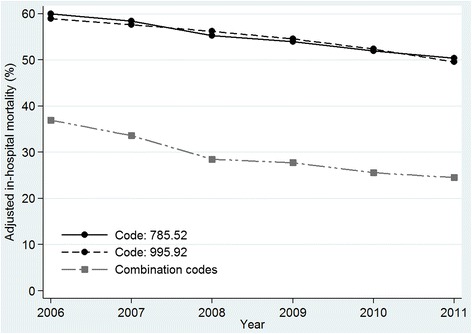
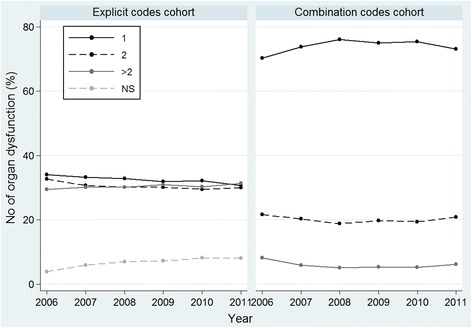
Results: Of 222 846 episodes of severe sepsis identified, 138 517 (62.2 %) were assigned explicit codes and 84 329 (37.8 %) combination codes; incidence rates were 60.6 and 36.9 cases per 100 000 inhabitants, respectively. Despite similar demographic characteristics, cases identified by explicit codes involved fewer comorbidities, fewer registered pathogens, greater extent of organ dysfunction (two or more organs affected in 60 % versus 26 % of cases) and higher in-hospital mortality (54.5 % versus 29 %; risk ratio 1.86, 95 % CI 1.83, 1.88). Between 2006 and 2011, explicit codes were increasingly implemented. Standardised incidence rates in this cohort increased over time with an APC of 12.3 % (95 % CI 4.4, 20.8); in the combination code cohort, rates increased by 3.8 % (95 % CI 1.3, 6.3). A decreasing trend in mortality was observed in both cohorts though the APC was -8.1 % (95 % CI -10.4, -5.7) in the combination code cohort and -3.5 % (95 % CI -3.9, -3.2) in the explicit code cohort.
Conclusions: Our findings suggest greater and increasing use of explicit codes for adult severe sepsis in Spain. This trend will have substantial impacts on epidemiological estimates, because these codes capture cases featuring greater organ dysfunction and in-hospital mortality.
Keywords: Epidemiology; Health services research; Incidence; Outcome; Severe sepsis; Trends.
Figures
Comment in
-
Sepsis and the theory of relativity: measuring a moving target with a moving measuring stick.Crit Care. 2016 Nov 21;20(1):396. doi: 10.1186/s13054-016-1559-z. Crit Care. 2016. PMID: 27923393 Free PMC article. No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
