

Extreme hypernatremia as a probable cause of fatal arrhythmia: a case report
- PMID: 27716387
- PMCID: PMC5045618
- DOI: 10.1186/s13256-016-1062-9
Extreme hypernatremia as a probable cause of fatal arrhythmia: a case report
Abstract
Background: Hypernatremia is a frequent occurrence among hospitalized patients. Severe hypernatremia is associated with mortality rates of over 60 %. Extreme hypernatremia, defined as sodium levels >190 mmol/l, is a rare occurrence. The literature on electrocardiographic changes occurring with this degree of hypernatremia is extremely scarce. We report the case of an 11-year-old Sri Lankan girl who presented with sodium levels of 226 mmol/l following infusion with 3 % hypertonic saline who developed diffuse QT prolongation leading to fatal ventricular tachycardia.
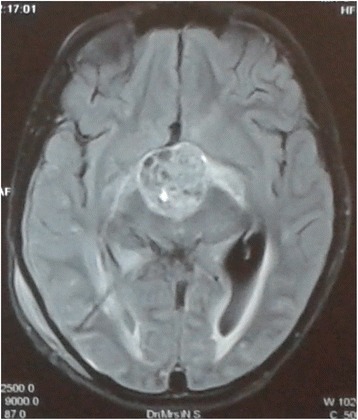
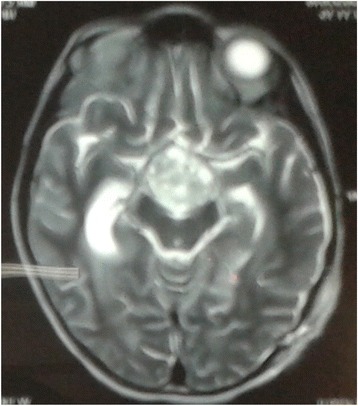
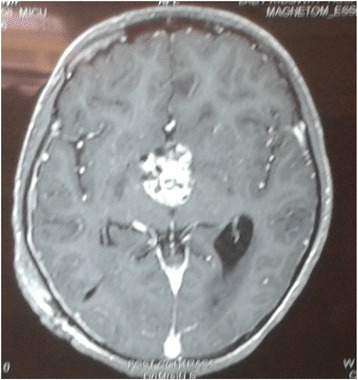
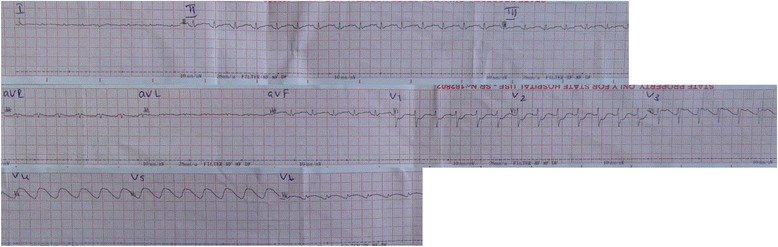
Case presentation: An 11-year-old Sri Lankan girl presented with fever, headache, vomiting, and altered level of consciousness. Following admission she developed generalized tonic-clonic seizures and was intubated and ventilated. She had a recent history of polyuria and polydipsia. Magnetic resonance imaging of her brain revealed hydrocephalus due to possible craniopharyngioma. A ventriculoperitoneal shunt was inserted and she was infused with 3 % hypertonic saline in an attempt to reduce intracranial pressure. The following day she became polyuric and dehydrated with tachycardia and low blood pressure. Biochemistry revealed serum sodium of 226 mmol/l, measured serum osmolality of 470 mOsm/kg, urine osmolality of 280 mOsm/kg, urine spot sodium of 116 mmol/l, blood urea of 8.1 mmol/l, and blood glucose of 8.5 mmol/l. Her serum potassium, calcium, and magnesium levels were normal. Extreme hypernatremia due to infusion of 3 % hypertonic saline in the background of cranial diabetes insipidus was considered. She was managed aggressively with 5 % dextrose infusion and clear water via nasogastric feeding to correct the fluid deficit of 7 liters over 36 hours. Her sodium levels dropped to 160 mmol/l the following day. However, she developed electrocardiographic changes with widespread gross QT prolongation with ST segment deviations followed by fatal ventricular tachycardia.
Conclusions: Extreme hypernatremia is rare, and the literature on electrocardiographic changes occurring at such high levels of sodium is scarce. At present there are no established guidelines on rate and mode of correction of such high sodium levels. This case highlights the electrocardiographic changes observed during extreme hypernatremia, controversies in managing increased intracranial pressure with hypertonic saline, and dilemmas encountered in managing extreme hypernatremia.
Keywords: Case report; ECG changes; Elevated intracranial pressure; Extreme hypernatremia; Hypertonic saline.
Figures
References
-
- Braun MM, Barstow CH, Pyzocha NJ. Diagnosing and management of sodium disorders: Hyponatremia and hypernatremia. Am Fam Physician. 2015;91(5):299–307. - PubMed
-
- Alshayeb HM, Showkat A, Babar F, et al. Severe hypernatremia correction rate and mortality in hospitalized patients. Am JMed Sci. 2011;341(5):356–60. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
