

A discrete cluster of urinary biomarkers discriminates between active systemic lupus erythematosus patients with and without glomerulonephritis
- PMID: 27716443
- PMCID: PMC5050957
- DOI: 10.1186/s13075-016-1120-0
A discrete cluster of urinary biomarkers discriminates between active systemic lupus erythematosus patients with and without glomerulonephritis
Abstract
Background: Management of lupus nephritis (LN) would be greatly aided by the discovery of biomarkers that accurately reflect changes in disease activity. Here, we used a proteomics approach to identify potential urinary biomarkers associated with LN.
Methods: Urine was obtained from 60 LN patients with paired renal biopsies, 25 active non-LN SLE patients, and 24 healthy controls. Using Luminex, 128 analytes were quantified and normalized to urinary creatinine levels. Data were analyzed by linear modeling and non-parametric statistics, with corrections for multiple comparisons. A second cohort of 33 active LN, 16 active non-LN, and 30 remission LN SLE patients was used to validate the results.
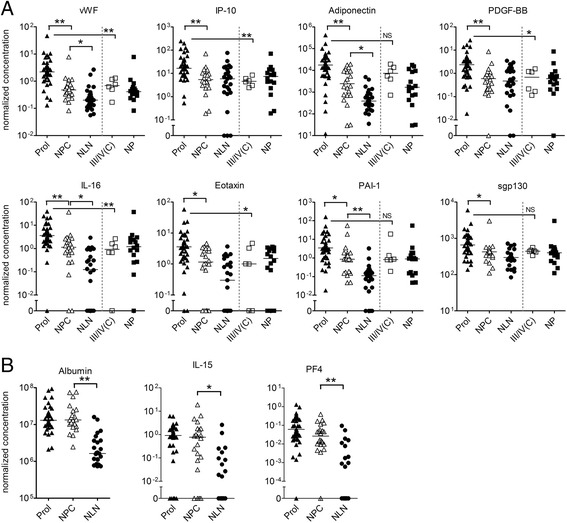
Results: Forty-four analytes were identified that were significantly increased in active LN as compared to active non-LN. This included a number of unique proteins (e.g., TIMP-1, PAI-1, PF4, vWF, and IL-15) as well as known candidate LN biomarkers (e.g., adiponectin, sVCAM-1, and IL-6), that differed markedly (>4-fold) between active LN and non-LN, all of which were confirmed in the validation cohort and normalized in remission LN patients. These proteins demonstrated an enhanced ability to discriminate between active LN and non-LN patients over several previously reported biomarkers. Ten proteins were found to significantly correlate with the activity score on renal biopsy, eight of which strongly discriminated between active proliferative and non-proliferative/chronic renal lesions.
Conclusions: A number of promising urinary biomarkers that correlate with the presence of active renal disease and/or renal biopsy changes were identified and appear to outperform many of the existing proposed biomarkers.
Keywords: Glomerulonephritis; Renal biopsy; Systemic lupus erythematosus; Urinary biomarkers.
Figures



References
-
- Rovin BH, Birmingham DJ, Nagaraja HN, Yu CY, Hebert LA. Biomarker discovery in human SLE nephritis. Bull NYU Hosp Jt Dis. 2007;65:187–93. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
