

Stratification of unresponsive patients by an independently validated index of brain complexity
- PMID: 27717082
- PMCID: PMC5132045
- DOI: 10.1002/ana.24779
Stratification of unresponsive patients by an independently validated index of brain complexity
Abstract
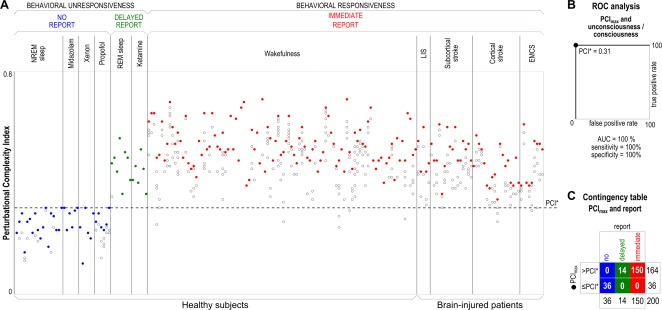
Objective: Validating objective, brain-based indices of consciousness in behaviorally unresponsive patients represents a challenge due to the impossibility of obtaining independent evidence through subjective reports. Here we address this problem by first validating a promising metric of consciousness-the Perturbational Complexity Index (PCI)-in a benchmark population who could confirm the presence or absence of consciousness through subjective reports, and then applying the same index to patients with disorders of consciousness (DOCs).
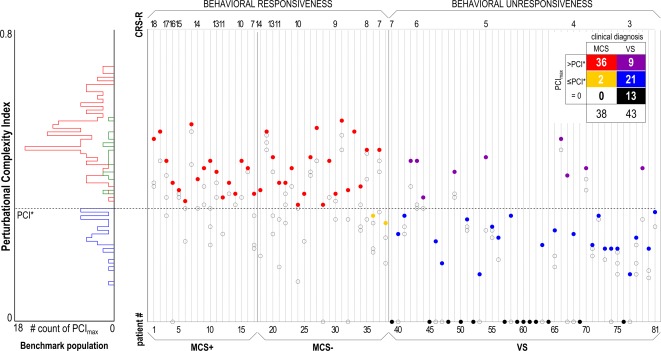
Methods: The benchmark population encompassed 150 healthy controls and communicative brain-injured subjects in various states of conscious wakefulness, disconnected consciousness, and unconsciousness. Receiver operating characteristic curve analysis was performed to define an optimal cutoff for discriminating between the conscious and unconscious conditions. This cutoff was then applied to a cohort of noncommunicative DOC patients (38 in a minimally conscious state [MCS] and 43 in a vegetative state [VS]).
Results: We found an empirical cutoff that discriminated with 100% sensitivity and specificity between the conscious and the unconscious conditions in the benchmark population. This cutoff resulted in a sensitivity of 94.7% in detecting MCS and allowed the identification of a number of unresponsive VS patients (9 of 43) with high values of PCI, overlapping with the distribution of the benchmark conscious condition.
Interpretation: Given its high sensitivity and specificity in the benchmark and MCS population, PCI offers a reliable, independently validated stratification of unresponsive patients that has important physiopathological and therapeutic implications. In particular, the high-PCI subgroup of VS patients may retain a capacity for consciousness that is not expressed in behavior. Ann Neurol 2016;80:718-729.
© 2016 The Authors. Annals of Neurology published by Wiley Periodicals, Inc. on behalf of American Neurological Association.
Figures
References
-
- Giacino JT, Kalmar K, Whyte J. The JFK Coma Recovery Scale‐Revised: measurement characteristics and diagnostic utility. Arch Phys Med Rehabil 2004;85:2020–2029. - PubMed
-
- Laureys S, Schiff ND. Coma and consciousness: paradigms (re)framed by neuroimaging. Neuroimage 2012;61:478–491. - PubMed
-
- Fernández‐Espejo D, Owen AM. Detecting awareness after severe brain injury. Nat Rev Neurosci 2013;14:801–809. - PubMed
-
- Fernández‐Espejo D, Rossit S, Owen AM. A thalamocortical mechanism for the absence of overt motor behavior in covertly aware patients. JAMA Neurol 2015;72:1442–1450. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
