

Disease Centered Around Calcified Taenia solium Granuloma
- PMID: 27720140
- PMCID: PMC5203955
- DOI: 10.1016/j.pt.2016.09.003
Disease Centered Around Calcified Taenia solium Granuloma
Abstract
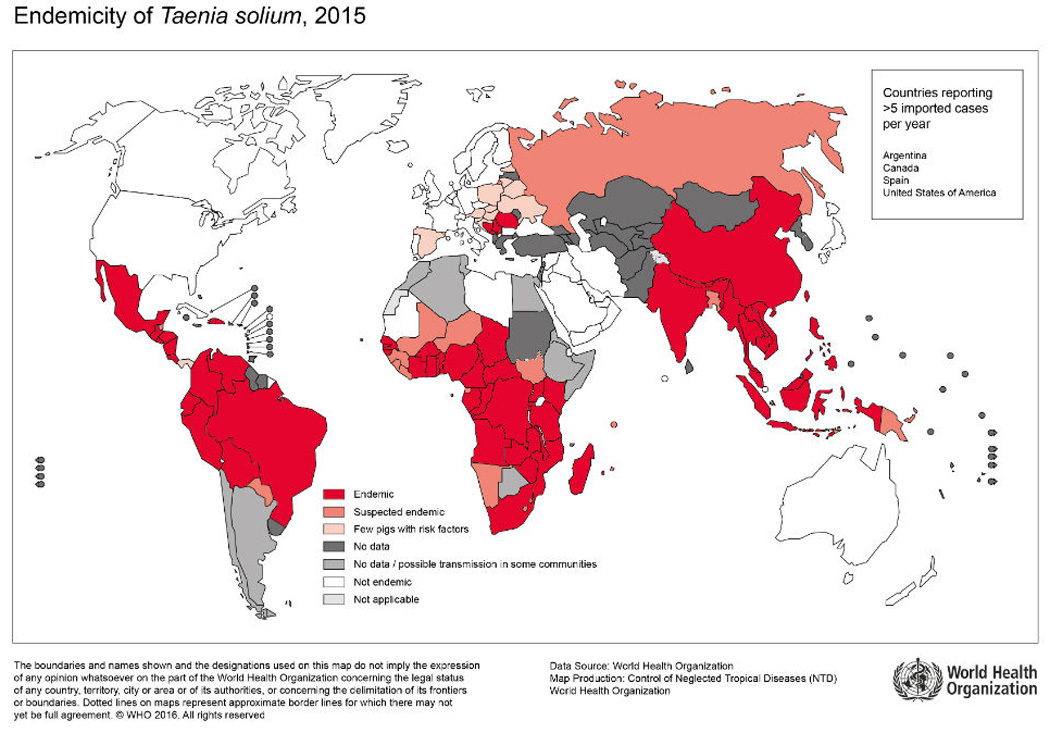
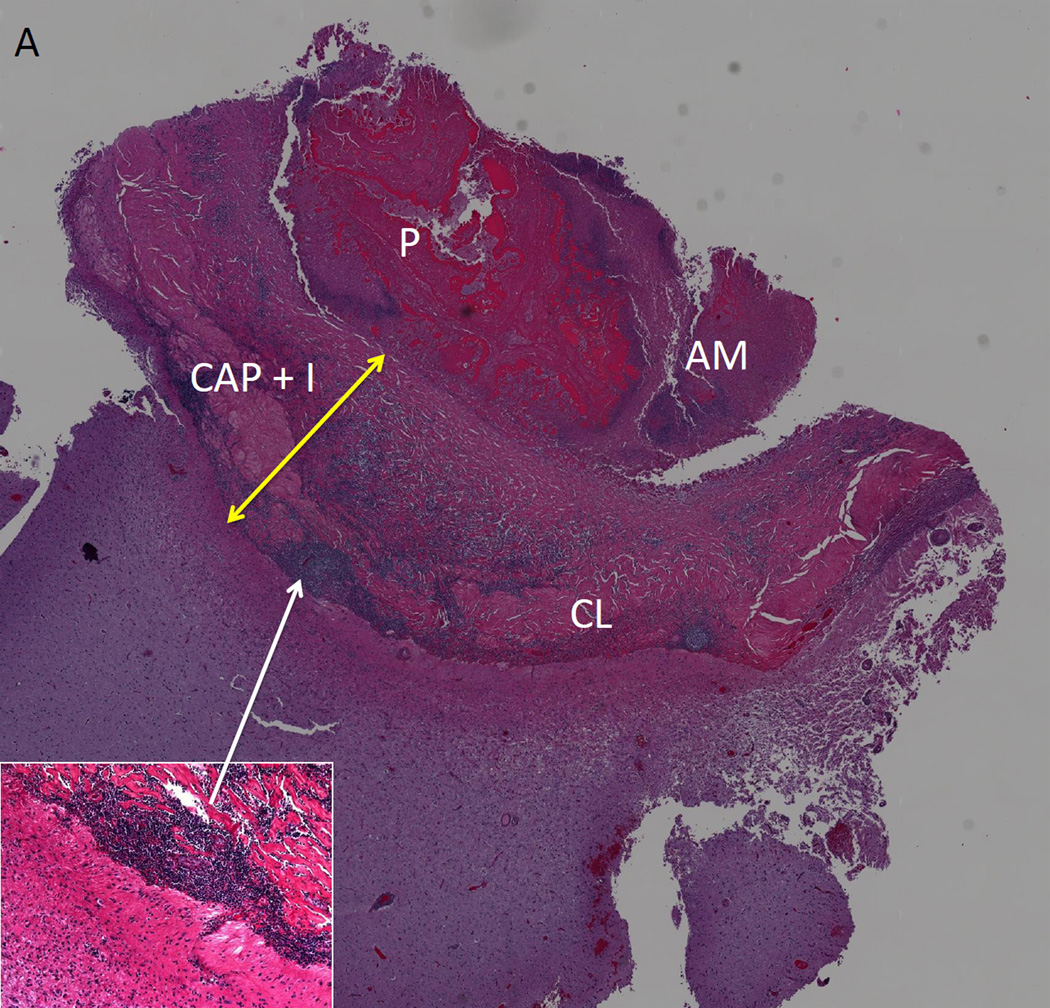
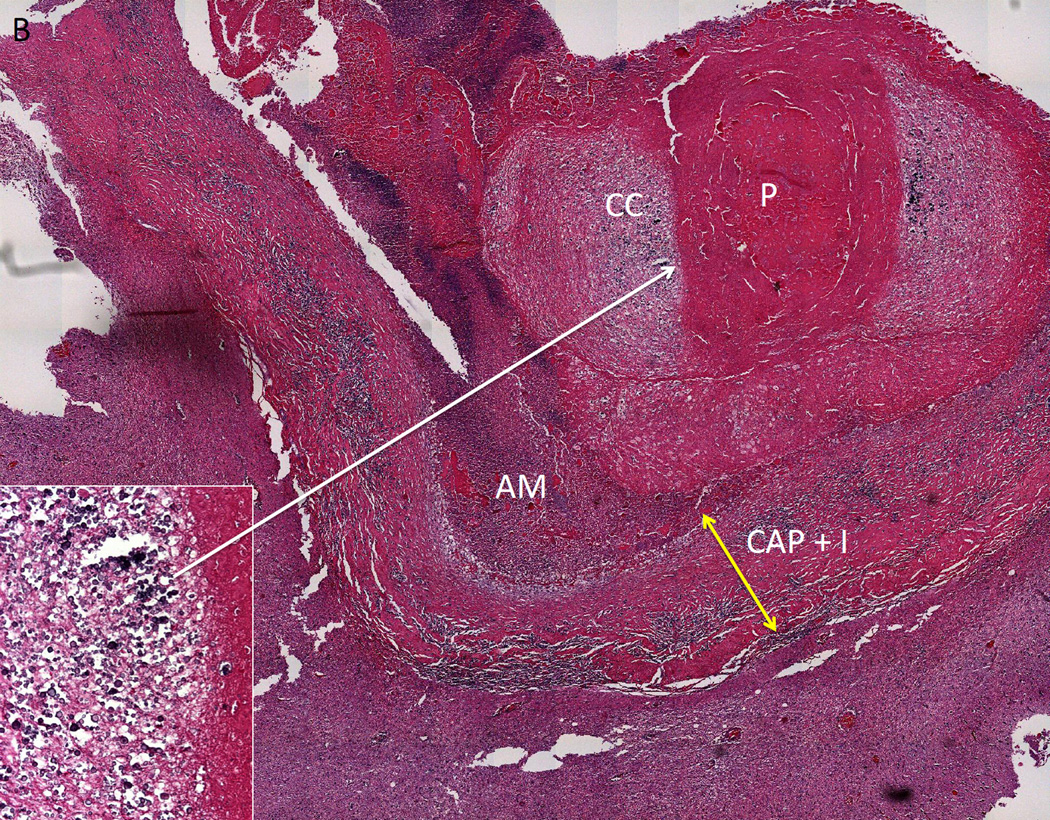
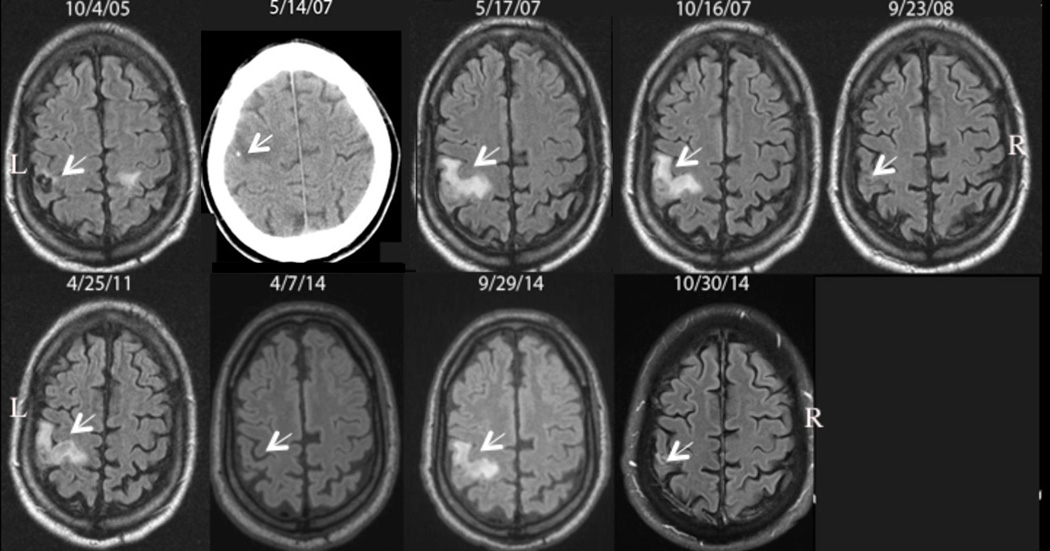
Taenia solium (the pork tapeworm) is present in most developing countries, where it is a frequent cause of seizures and other neurological disease. Parasitic larvae invade the human brain, establish, and eventually resolve, leaving a calcified scar. While these lesions are common in endemic regions, and most of these are clinically silent, a proportion of individuals with calcified cysticerci develop seizures from these lesions, and 30-65% of these cases are associated with perilesional edema (PE), likely due to host inflammation. This manuscript summarizes the importance, characteristics, natural history, and potential prevention and treatments of symptomatic calcified neurocysticercosis (NCC).
Keywords: calcified granuloma; epilepsy; neurocysticercosis; perilesional edema; seizures.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Figures
References
-
- Garcia HH, Del Brutto OH. Neurocysticercosis: updated concepts about an old disease. The Lancet. Neurology. 2005;4:653–661. - PubMed
-
- Newton CR, Garcia HH. Epilepsy in poor regions of the world. Lancet. 2012;380:1193–1201. - PubMed
-
- Schantz PM. Taenia solium cysticercosis: an overview of global distribution and transmission. In: Singh G, Prabhakar S, editors. Taenia solium cysticercosis : from basic to clinical science. CABI Pub; 2002. pp. 63–73.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
