

Mortality Among Men with Advanced Prostate Cancer Excluded from the ProtecT Trial
- PMID: 27720537
- PMCID: PMC5289293
- DOI: 10.1016/j.eururo.2016.09.040
Mortality Among Men with Advanced Prostate Cancer Excluded from the ProtecT Trial
Abstract
Background: Early detection and treatment of asymptomatic men with advanced and high-risk prostate cancer (PCa) may improve survival rates.
Objective: To determine outcomes for men diagnosed with advanced PCa following prostate-specific antigen (PSA) testing who were excluded from the ProtecT randomised trial.
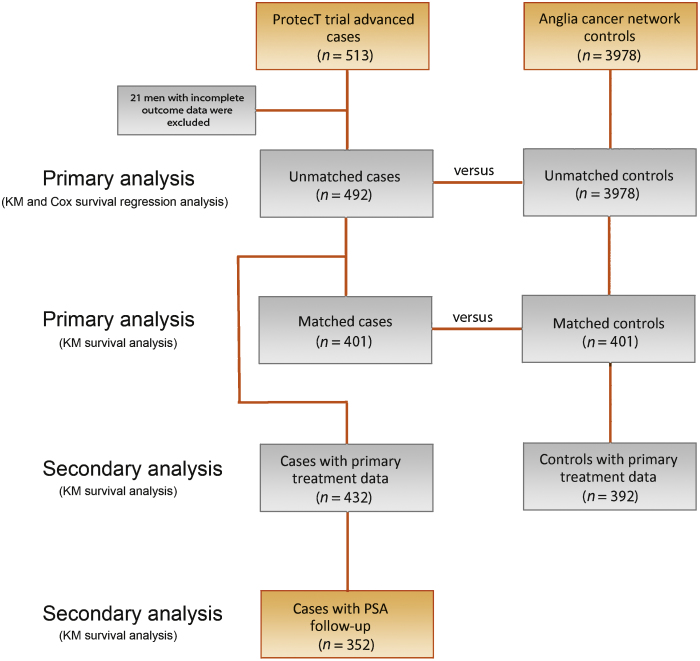
Design, setting, and participants: Mortality was compared for 492 men followed up for a median of 7.4 yr to a contemporaneous cohort of men from the UK Anglia Cancer Network (ACN) and with a matched subset from the ACN.
Outcome measurements and statistical analysis: PCa-specific and all-cause mortality were compared using Kaplan-Meier analysis and Cox's proportional hazards regression.
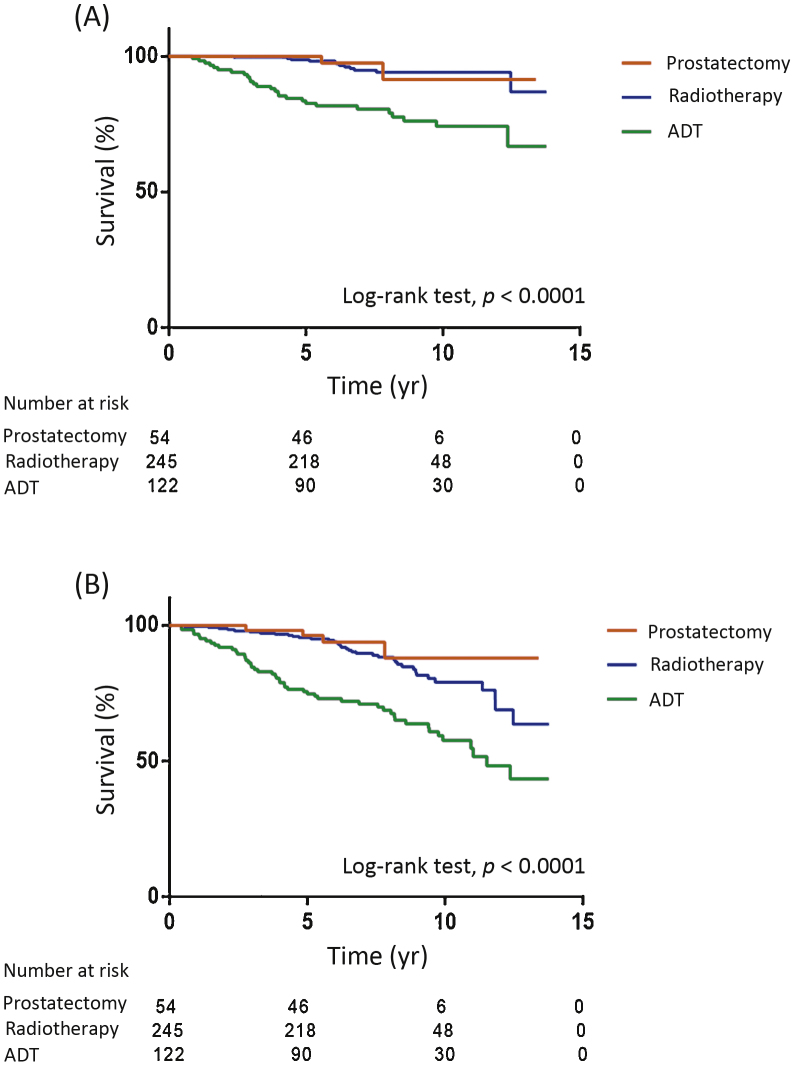
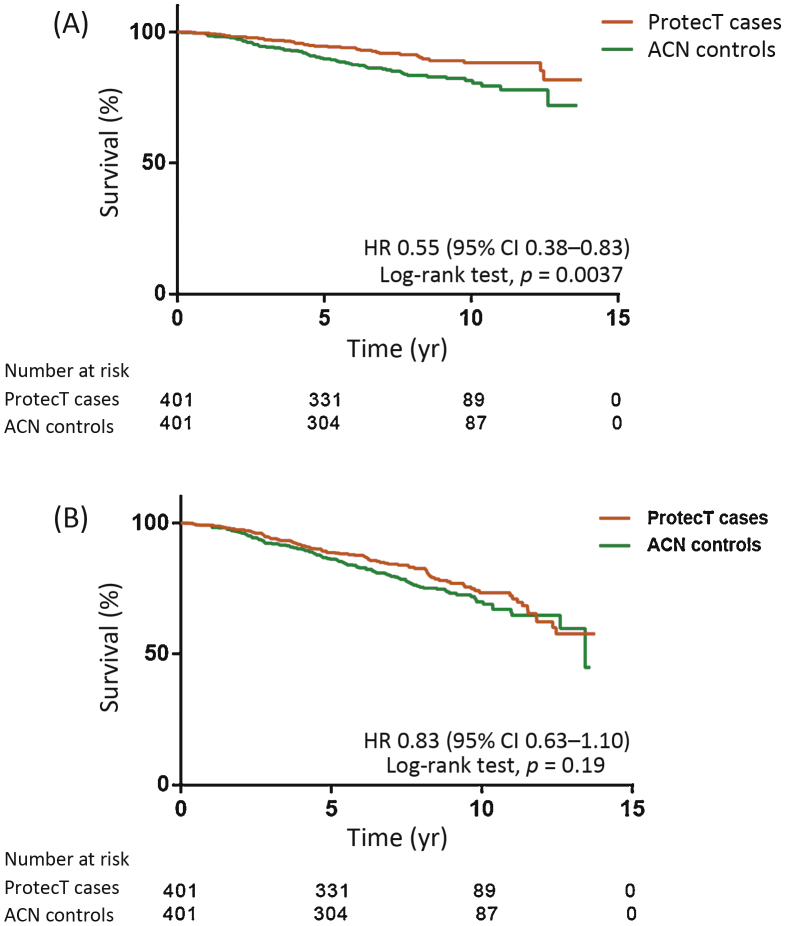
Results and limitations: Of the 492 men excluded from the ProtecT cohort, 37 (8%) had metastases (N1, M0=5, M1=32) and 305 had locally advanced disease (62%). The median PSA was 17μg/l. Treatments included radical prostatectomy (RP; n=54; 11%), radiotherapy (RT; n=245; 50%), androgen deprivation therapy (ADT; n=122; 25%), other treatments (n=11; 2%), and unknown (n=60; 12%). There were 49 PCa-specific deaths (10%), of whom 14 men had received radical treatment (5%); and 129 all-cause deaths (26%). In matched ProtecT and ACN cohorts, 37 (9%) and 64 (16%), respectively, died of PCa, while 89 (22%) and 103 (26%) died of all causes. ProtecT men had a 45% lower risk of death from PCa compared to matched cases (hazard ratio 0.55, 95% confidence interval 0.38-0.83; p=0.0037), but mortality was similar in those treated radically. The nonrandomised design is a limitation.
Conclusions: Men with PSA-detected advanced PCa excluded from ProtecT and treated radically had low rates of PCa death at 7.4-yr follow-up. Among men who underwent nonradical treatment, the ProtecT group had a lower rate of PCa death. Early detection through PSA testing, leadtime bias, and group heterogeneity are possible factors in this finding.
Patient summary: Prostate cancer that has spread outside the prostate gland without causing symptoms can be detected via prostate-specific antigen testing and treated, leading to low rates of death from this disease.
Keywords: Prostate cancer; Prostate-specific antigen screening; Survival.
Copyright © 2016 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
What Early ProtecT Results Have Confirmed About Risk-stratified Prostate Cancer Management.Eur Urol. 2017 Mar;71(3):389-390. doi: 10.1016/j.eururo.2016.10.017. Epub 2016 Nov 1. Eur Urol. 2017. PMID: 27815085 No abstract available.
-
Re: Mortality among Men with Advanced Prostate Cancer Excluded from the ProtecT Trial.J Urol. 2017 Jun;197(6):1456-1457. doi: 10.1016/j.juro.2017.03.053. Epub 2017 Mar 15. J Urol. 2017. PMID: 28505898 No abstract available.
References
-
- Shoag J.E., Mittal S., Hu J.C. Reevaluating PSA testing rates in the PLCO trial. N Engl J Med. 2016;374:1795–1796. - PubMed
-
- Widmark A., Klepp O., Solberg A. Endocrine treatment, with or without radiotherapy, in locally advanced prostate cancer (SPCG-7/SFUO-3): an open randomised phase III trial. Lancet. 2009;373:301–308. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
