Risk factors of delayed diagnosis of acute appendicitis in children: for early detection of acute appendicitis
- PMID: 27721841
- PMCID: PMC5052135
- DOI: 10.3345/kjp.2016.59.9.368
Risk factors of delayed diagnosis of acute appendicitis in children: for early detection of acute appendicitis
Abstract
Purpose: This study examined the risk factors of a delayed diagnosis of acute appendicitis in children undergoing an appendectomy.
Methods: This retrospective study involved children aged below 18 years, who underwent an appendectomy. After dividing them into a delayed diagnosis group and nondelayed diagnosis group according to the time interval between the initial hospital visit and final diagnosis, the risk factors of delayed diagnosis were identified using logistic regression analysis.
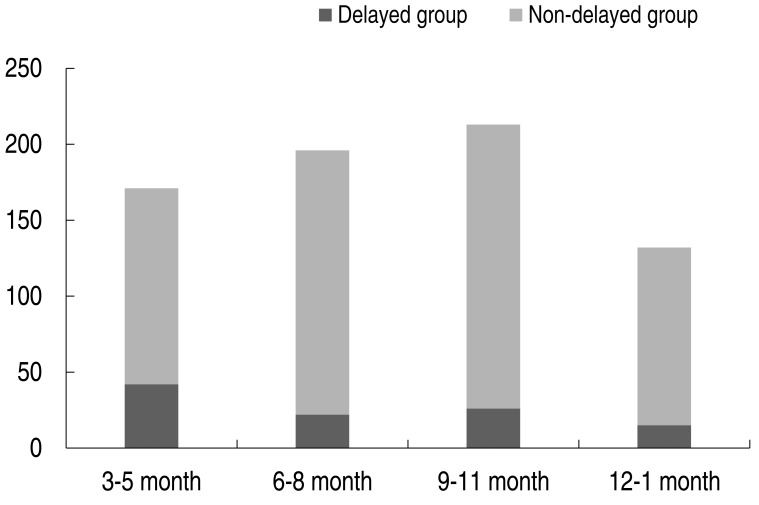
Results: Among 712 patients, 105 patients (14.7%) were classified in the delayed diagnosis group; 92 patients (12.9%) were diagnosed using ultrasonography (US), and both US and computed tomography were performed in 38 patients (5.3%). More patients in the delayed diagnosis group underwent US (P=0.03). Spring season and prior local clinic visit were significantly associated with a delayed diagnosis. Fever and diarrhea were more common in the delayed diagnosis group (fever: odds ratio [OR], 1.37; 95% confidence interval [CI], 1.05-1.81; diarrhea: OR, 1.94; 95% CI, 1.08-3.46; P<0.05). These patients showed symptoms for a longer duration (OR, 2.59; 95% CI, 1.78-3.78; P<0.05), and the admission course (OR, 1.26; 95% CI, 1.11-1.44; P<0.05) and C-reactive protein (CRP) levels (OR, 1.47; 95% CI, 1.19-1.82; P<0.05) were associated with the delayed diagnosis.
Conclusion: To decrease the rate of delayed diagnoses of acute appendicitis, symptoms such as fever and diarrhea, seasonal variations, admission course, and CRP levels should be considered and children with a longer duration of symptoms should be closely monitored.
Keywords: Appendicitis; Child; Delayed diagnosis; Risk factors.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Factors Associated With Potentially Missed Diagnosis of Appendicitis in the Emergency Department.JAMA Netw Open. 2020 Mar 2;3(3):e200612. doi: 10.1001/jamanetworkopen.2020.0612. JAMA Netw Open. 2020. PMID: 32150270 Free PMC article.
-
Ultrasound, computed tomography, and laboratory findings in the diagnosis of appendicitis.Acta Radiol. 2007 Apr;48(3):267-73. doi: 10.1080/02841850601182162. Acta Radiol. 2007. PMID: 17453494
-
Hospital type predicts computed tomography use for pediatric appendicitis.J Pediatr Surg. 2019 Apr;54(4):723-727. doi: 10.1016/j.jpedsurg.2018.05.018. Epub 2018 May 29. J Pediatr Surg. 2019. PMID: 29925468
-
Selective imaging strategies for the diagnosis of appendicitis in children.Pediatrics. 2004 Jan;113(1 Pt 1):24-8. doi: 10.1542/peds.113.1.24. Pediatrics. 2004. PMID: 14702442
-
Increased risk of neoplasm in appendicitis treated with interval appendectomy: single-institution experience and literature review.Am Surg. 2012 Mar;78(3):339-43. Am Surg. 2012. PMID: 22524774 Review.
Cited by
-
A clinically-guided unsupervised clustering approach to recommend symptoms of disease associated with diagnostic opportunities.Diagnosis (Berl). 2022 Sep 21;10(1):43-53. doi: 10.1515/dx-2022-0044. eCollection 2023 Feb 1. Diagnosis (Berl). 2022. PMID: 36127310 Free PMC article.
-
Complicated appendicitis and associated risk factors among children.BMC Pediatr. 2025 Apr 29;25(1):336. doi: 10.1186/s12887-025-05447-5. BMC Pediatr. 2025. PMID: 40301796 Free PMC article.
-
Time between onset of symptoms and definitive treatment in children with acute appendicitis: How it affects length of hospital stay?Afr J Paediatr Surg. 2022 Oct-Dec;19(4):245-250. doi: 10.4103/ajps.ajps_67_21. Afr J Paediatr Surg. 2022. PMID: 36018207 Free PMC article.
-
Predictors of complicated appendicitis among patients presented to public referral hospitals in Harari region, Eastern Ethiopia: a case-control study.Surg Pract Sci. 2022 Mar 14;9:100072. doi: 10.1016/j.sipas.2022.100072. eCollection 2022 Jun. Surg Pract Sci. 2022. PMID: 39845075 Free PMC article.
-
Acute Appendicitis in Young Children: A Persistent Diagnostic Challenge for Clinicians.Cureus. 2018 Mar 19;10(3):e2347. doi: 10.7759/cureus.2347. Cureus. 2018. PMID: 29796359 Free PMC article.
References
-
- Pittman-Waller VA, Myers JG, Stewart RM, Dent DL, Page CP, Gray GA, et al. Appendicitis: why so complicated? Analysis of 5755 consecutive appendectomies. Am Surg. 2000;66:548–554. - PubMed
-
- Rothrock SG, Pagane J. Acute appendicitis in children: emergency department diagnosis and management. Ann Emerg Med. 2000;36:39–51. - PubMed
-
- Rothrock SG, Skeoch G, Rush JJ, Johnson NE. Clinical features of misdiagnosed appendicitis in children. Ann Emerg Med. 1991;20:45–50. - PubMed
-
- Curran TJ, Muenchow SK. The treatment of complicated appendicitis in children using peritoneal drainage: results from a public hospital. J Pediatr Surg. 1993;28:204–208. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous