

Effect of tracheostomy tube on work of breathing: Comparison of pre- and post-decannulation
- PMID: 27722109
- PMCID: PMC5051063
- DOI: 10.4103/2229-5151.190651
Effect of tracheostomy tube on work of breathing: Comparison of pre- and post-decannulation
Abstract
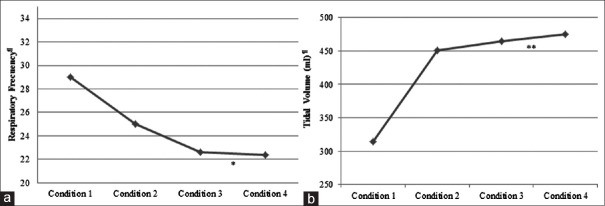
Objective: To describe and compare the work of breathing (WOB) during spontaneous breathing under four conditions: (1) breathing through a tracheostomy tube with an inflated cuff, (2) breathing through the upper airway (UA) with a deflated cuff and occluded tube, (3) breathing through the UA with an occluded cuffless tube, and (4) postdecannulation.
Patients and methods: Patients who tolerated an occluded cuffless tube were included. Ventilatory variables and esophageal pressure were recorded. The pressure-time product (PTP), PTP/min, and PTP/min/tidal volume (PTP/min/VT) were measured. Each condition was measured for 5 min with a 15 min time interval between evaluations. Quantitative data are expressed as mean ± standard deviation. Single-factor analysis of variance was used, and the Games-Howell test was used for post hoc analysis of comparisons between group means (P ≤ 0.05).
Results: Eight patients were studied under each of the four conditions described above. Statistically significant differences were found for PTP, PTP/min, and PTP/min/VT. In the post hoc analysis for PTP, significant differences among all conditions were found. For PTP/min, there was no significant difference between Conditions 2 and 4 (P = 0.138), and for PTP/min/VT, there was no significant difference between Conditions 1 and 2 (P = 0.072) or between Conditions 2 and 3 (P = 0.106). A trend toward a higher PTP, PTP/min, and PTP/min/VT was observed when breathing through a cuffless tracheostomy tube.
Conclusion: The four conditions differed with respect to WOB. Cuff inflation could result in a reduced WOB because there is less dead space. Cuffless tracheostomy tubes generate increased WOB, perhaps due to the material deformity caused by body temperature.
Keywords: Airway care; airway extubation; artificial airway; decannulation; extubation methods; tracheostomy; work of breathing.
Figures

References
-
- Villalba D, Plotnikow G, Feld V, Rivero Vairo N, Scapellato J, Díaz Nielsen E. Weaning from prolonged mechanical ventilation at 72 hours of spontaneous breathing. Medicina (B Aires) 2015;75:11–7. - PubMed
-
- Scrigna M, Plotnikow G, Feld V, Villalba D, Quiroga C, Leiva V, et al. Decannulation after the ICU Stay. Analysis of 181 Tracheostomized Patients Rev Am Med Respir. 2013;13(2):58–63.
-
- Rumbak MJ, Graves AE, Scott MP, Sporn GK, Walsh FW, Anderson WM, et al. Tracheostomy tube occlusion protocol predicts significant tracheal obstruction to airflow in patients requiring prolonged mechanical ventilation. Crit Care Med. 1997;25:413–7. - PubMed
-
- Beard B, Monaco F. Tracheostomy discontinuation: Impact of tube selection on resistance during tube occlusion. Respir Care. 1993;38:267–70.
-
- Hussey JD, Bishop MJ. Pressures required to move gas through the native airway in the presence of a fenestrated vs a nonfenestrated tracheostomy tube. Chest. 1996;110:494–7. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
