

Craniofacial features as assessed by lateral cephalometric measurements in children with Down syndrome
- PMID: 27722998
- PMCID: PMC5097953
- DOI: 10.1186/s40510-016-0148-7
Craniofacial features as assessed by lateral cephalometric measurements in children with Down syndrome
Abstract
Objective: The objective of the present study is to examine the craniofacial development of patients with Down syndrome (DS) and compare them with a neurotypical population.
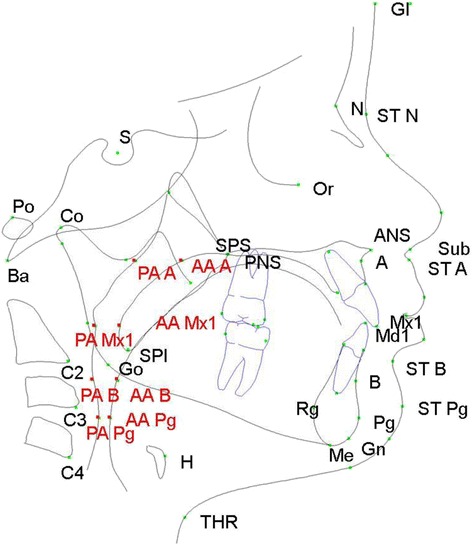
Methods: This study is a cross-sectional analysis of lateral cephalometric radiographs of participants with DS. The study population consisted of children and young adults with DS aged 3-25 years. Cephalometric data were summarized by age and sex. Raw and normalized z-scores were computed. One-sample t tests were used to test whether mean z-scores differed from zero. The demographic characteristics between those with or without lateral cephalograms among all study participants were compared by Fisher's exact tests.
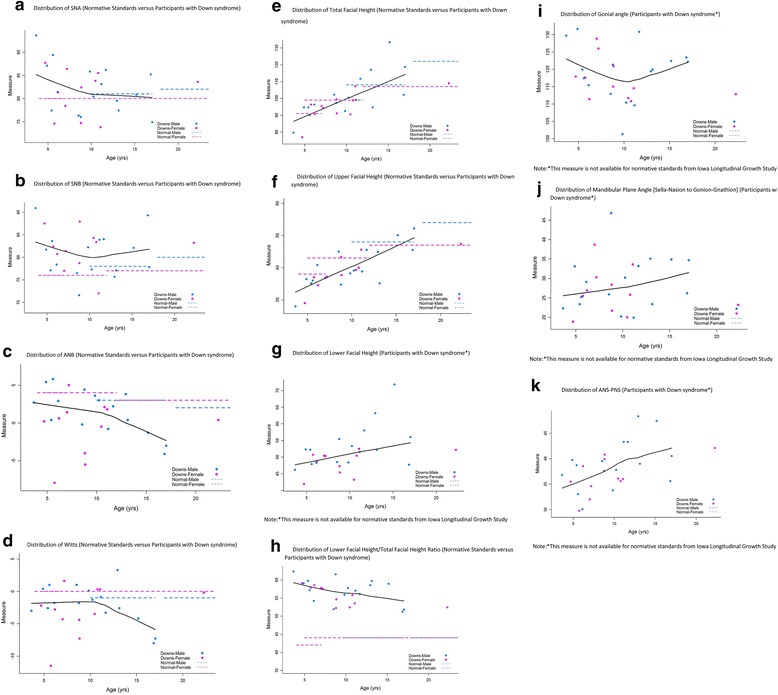
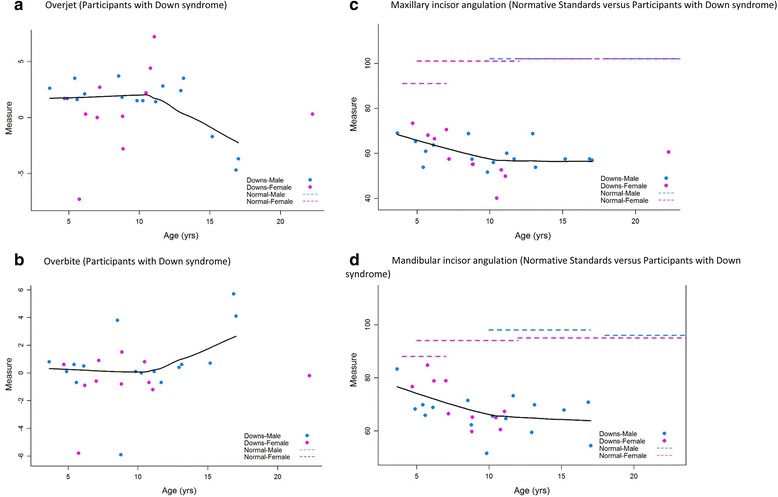
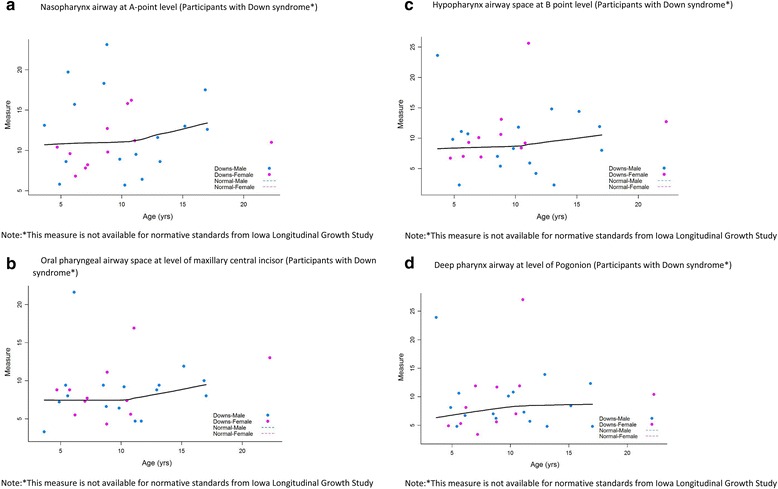
Results: The study sample comprised of 27 participants with DS. Study subjects demonstrated a class III skeletal pattern. This was more pronounced in the older age groups as compared to younger age groups. Subjects also had an increased proportionate lower anterior face height to total facial height compared to normative standards. Gonial angles, mandibular plane angles, and airway measurements increased with age.
Conclusions: Patients with Down syndrome present typically with class III skeletal pattern and long lower anterior facial heights. In patients with Down syndrome, comprehensive phase of orthodontic treatment may be best initiated following cessation of growth.
Figures
References
-
- Gorlin RJ, Cohen MM, Levin LS. Syndromes of the head and neck. 4. New York, NY: Oxford University Press; 2001. pp. 35–42.
-
- Stoll C, Alembik Y, Dott B, Roth MP. Study of Down syndrome in 238,942 consecutive births. Ann Genet. 1998;41(1):44–51. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
