

Impact of symptom burden and health-related quality of life (HRQOL) on esophageal motor diagnoses
- PMID: 27723241
- PMCID: PMC5367979
- DOI: 10.1111/nmo.12970
Impact of symptom burden and health-related quality of life (HRQOL) on esophageal motor diagnoses
Abstract
Background: High-resolution manometry (HRM) categorizes esophageal motor processes into specific Chicago Classification (CC) diagnoses, but the clinical impact of these motor diagnoses on symptom burden remain unclear.
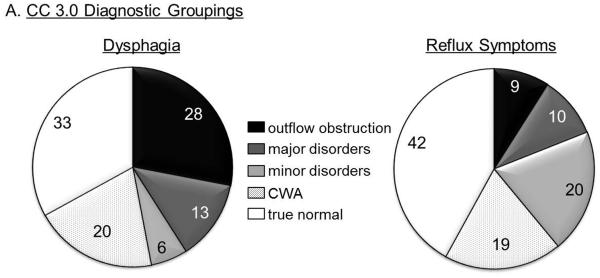
Methods: Two hundred and eleven subjects (56.8±1.0 years, 66.8% F) completed symptom questionnaires (GERDQ, Mayo dysphagia questionnaire [MDQ], visceral sensitivity index, short-form 36, dominant symptom index, and global symptom severity [GSS] on a 100-mm visual analog scale) prior to HRM. Subjects were stratified according to CC v3.0 and by dominant presenting symptom; contraction wave abnormalities (CWA) were evaluated within "normal" CC. Symptom burden, impact of diagnoses, and HRQOL were compared within and between cohorts.
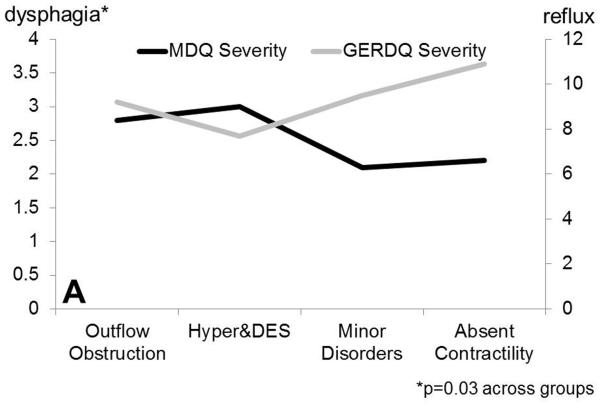
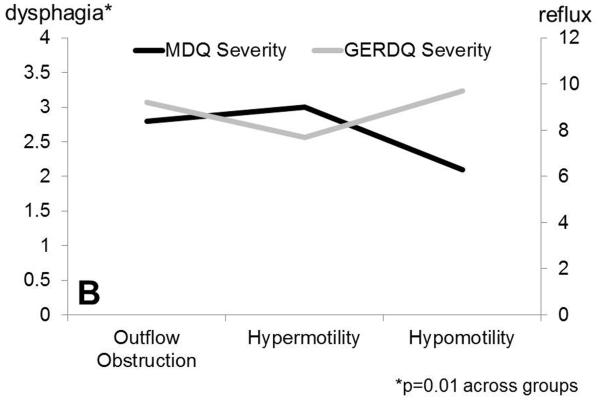
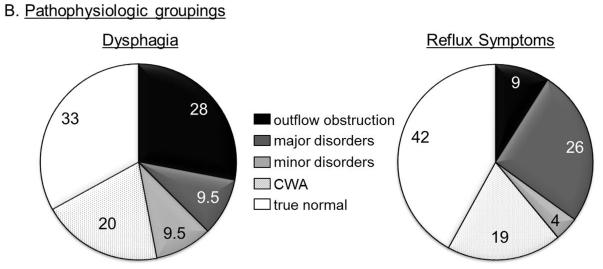
Key results: Major motor disorders had highest global symptom burden (P=.02), "normal" had lowest (P<.01). Dysphagia (MDQ) was highest with esophageal outflow obstruction (P=.02), but reflux symptoms (GERDQ) were similar in CC cohorts (P=ns). Absent contractility aligned best with minor motor disorders. Consequently, pathophysiologic categorization into outflow obstruction, hypermotility, and hypomotility resulted in a gradient of decreasing dysphagia and increasing reflux burden (P<.05 across groups); GSS (P=.05) was highest with hypomotility and lowest with "normal" (P=.002). Within the "normal" cohort, 33.3% had CWA; this subgroup had symptom burden similar to hypermotility. Upon stratification by symptoms, symptom burden (GSS, MDQ, HRQOL) was most profound with dysphagia.
Conclusions and inferences: Chicago Classification v3.0 diagnoses identify subjects with highest symptom burden, but pathophysiologic categorization may allow better stratification by symptom type and burden. Contraction wave abnormalities are clinically relevant and different from true normal motor function. Transit symptoms have highest yield for a motor diagnosis.
Keywords: Chicago Classification; dysphagia; high-resolution manometry; symptom burden.
© 2016 John Wiley & Sons Ltd.
Figures
References
-
- Gyawali CP, Bredenoord AJ, Conklin JL, et al. Evaluation of esophageal motor function in clinical practice. Neurogastroenterol Motil. 2013;25:99–133. - PubMed
-
- Chan WW, Haroian LR, Gyawali CP. Value of preoperative esophageal function studies before laparoscopic antireflux surgery. Surg Endosc. 2011;25:2943–9. - PubMed
-
- Teitelbaum EN, Soper NJ, Santos BF, et al. Symptomatic and physiologic outcomes one year after peroral esophageal myotomy (POEM) for treatment of achalasia. Surg Endosc. 2014;28:3359–65. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
