

Prevalence of pain 6 months after surgery: a prospective observational study
- PMID: 27724844
- PMCID: PMC5057259
- DOI: 10.1186/s12871-016-0261-7
Prevalence of pain 6 months after surgery: a prospective observational study
Abstract
Background: Pain after surgery is a major issue for patient discomfort and often associated with delayed recovery. The aim of the present study was to evaluate the prevalence of pain and requirement for analgesics up to 6 months after elective surgery, independent if new pain symptoms occurred after surgery or if preoperative pain persisted in the postoperative period.
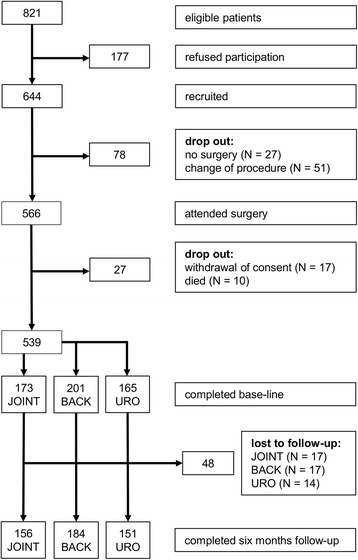
Methods: A prospective observational single center cohort study was conducted between January 2012 and August 2013. Eligible patients were scheduled to undergo elective surgical interventions including joint (hip, knee arthroplasty), back (nucleotomy, spondylodesis), or urological surgery (cystectomy, prostatectomy, nephrectomy). Pain was assessed on an 11-point numerical rating scale (NRS) before, on postoperative day 2 and 6 months after surgery. Clinical information was collected with structured questionnaires and by telephone interview.
Results: Six hundred and forty-four patients gave informed consent, including 54.4 % men (mean age 62.2, SD 14.3). Higher preoperative pain scores were found in patients undergoing joint (mean 7.6; 95 % confidence interval [CI]: 7.2-8.0) and back surgery (mean 7.1, CI: 6.8-7.5) than in patients prior to urological surgery (mean 2.3; CI: 1.8-2.8). After 6 months, about 50 % of patients after joint or back surgery indicated pain levels ≥3/10, compared to 15.9 % of patients after urological surgery (p < .001). 35.3 % of the patients after joint surgery and 41.3 % after back surgery still use pain medication 6 months postoperatively, in contrast to 7.3 % of patients after urological surgery. 13.6 % of patients who underwent back surgery indicated the regular intake of opioids.
Conclusions: Our results reveal that a significant percentage of patients undergoing procedures in joint or back surgery still need pain medication up to 6 months postoperatively due to ongoing pain symptoms. Improved monitoring of pain management is warranted, especially after discharge from hospital, to improve long-term results.
Trial registration: Clinicaltrials.gov (Identifier: NCT01488617 ); date of registration December 6th 2011.
Keywords: Analgesics; Chronic pain; Outcome; Postoperative pain.
Figures

References
-
- S3-Leitlinie Behandlung akuter perioperativer und posttraumatischer Schmerzen. Deutsche Interdisziplinäre Vereinigung für Schmerztherapie (DIVS). Deutscher Ärzte-Verlag, Köln. AWMF-Register Nr. 041/001; 2007/05/21 [cited 2016/02/21]; Available from: http://www.awmf.org/.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
