

Evaluation of Esophageal Motility Utilizing the Functional Lumen Imaging Probe
- PMID: 27725650
- PMCID: PMC5224528
- DOI: 10.1038/ajg.2016.454
Evaluation of Esophageal Motility Utilizing the Functional Lumen Imaging Probe
Abstract
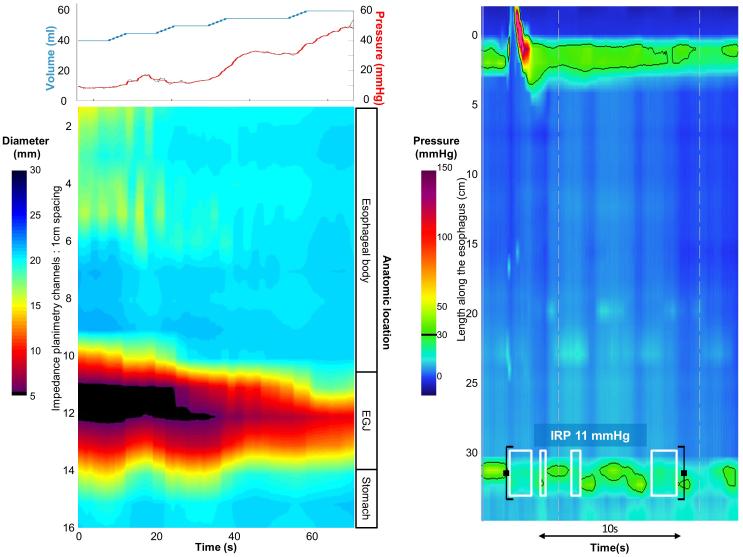
Objectives: Esophagogastric junction (EGJ) distensibility and distension-mediated peristalsis can be assessed with the functional lumen imaging probe (FLIP) during a sedated upper endoscopy. We aimed to describe esophageal motility assessment using FLIP topography in patients presenting with dysphagia.
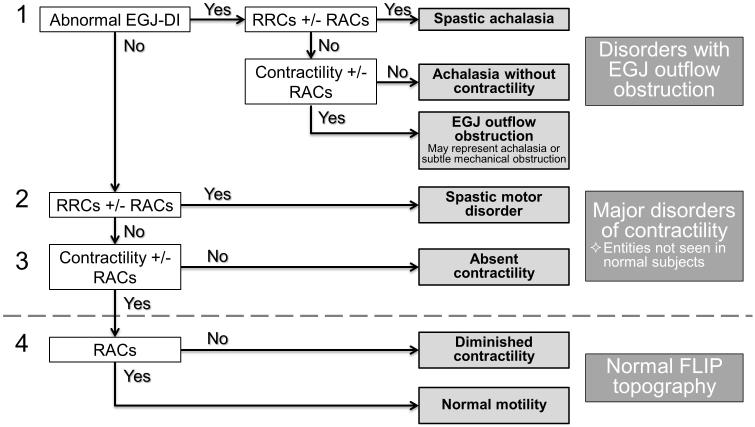
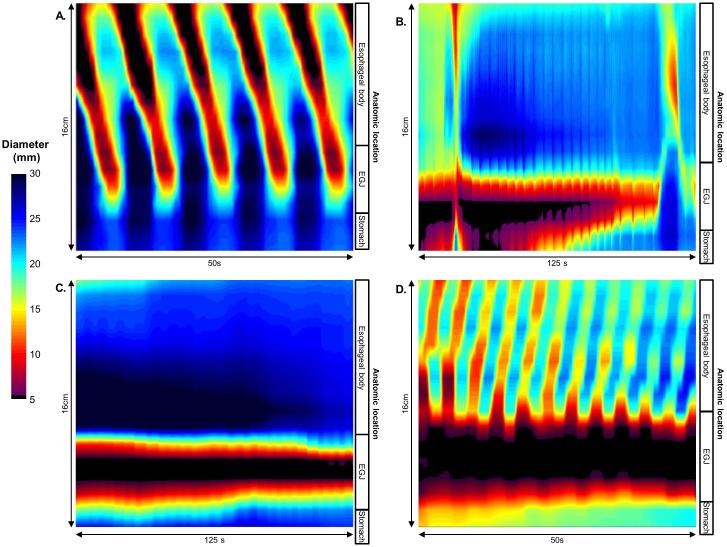
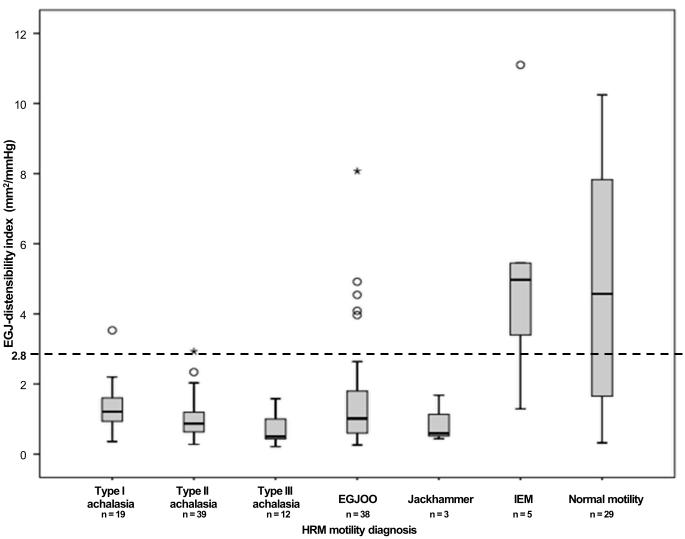
Methods: In all, 145 patients (aged 18-85 years, 54% female) with dysphagia that completed upper endoscopy with a 16-cm FLIP assembly and high-resolution manometry (HRM) were included. HRM was analyzed according to the Chicago Classification of esophageal motility disorders; major esophageal motility disorders were considered "abnormal". FLIP studies were analyzed using a customized program to calculate the EGJ-distensibility index (DI) and generate FLIP topography plots to identify esophageal contractility patterns. FLIP topography was considered "abnormal" if EGJ-DI was <2.8 mm2/mm Hg or contractility pattern demonstrated absent contractility or repetitive, retrograde contractions.
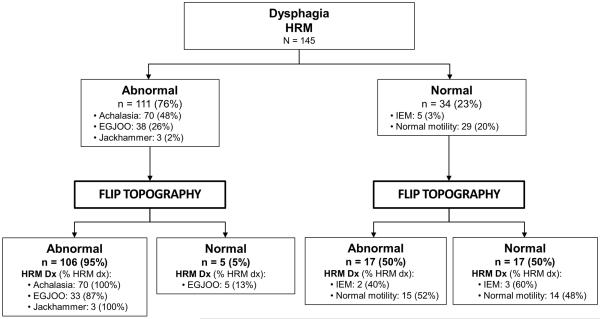
Results: HRM was abnormal in 111 (77%) patients: 70 achalasia (19 type I, 39 type II, and 12 type III), 38 EGJ outflow obstruction, and three jackhammer esophagus. FLIP topography was abnormal in 106 (95%) of these patients, including all 70 achalasia patients. HRM was "normal" in 34 (23%) patients: five ineffective esophageal motility and 29 normal motility. In all, 17 (50%) had abnormal FLIP topography including 13 (37%) with abnormal EGJ-DI.
Conclusions: FLIP topography provides a well-tolerated method for esophageal motility assessment (especially to identify achalasia) at the time of upper endoscopy. FLIP topography findings that are discordant with HRM may indicate otherwise undetected abnormalities of esophageal function, thus FLIP provides an alternative and complementary method to HRM for evaluation of non-obstructive dysphagia.
Figures
References
-
- Rohof WO, Hirsch DP, Kessing BF, et al. Efficacy of treatment for patients with achalasia depends on the distensibility of the esophagogastric junction. Gastroenterology. 2012;143(2):328–35. - PubMed
-
- Smeets FG, Masclee AA, Keszthelyi D, et al. Esophagogastric junction distensibility in the management of achalasia patients: relation to treatment outcome. Neurogastroenterol Motil. 2015;27(10):1495–503. - PubMed
-
- Orvar KB, Gregersen H, Christensen J. Biomechanical characteristics of the human esophagus. Dig Dis Sci. 1993;38(2):197–205. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
