

Comparison of stapled haemorrhoidopexy with traditional excisional surgery for haemorrhoidal disease (eTHoS): a pragmatic, multicentre, randomised controlled trial
- PMID: 27726951
- PMCID: PMC5269572
- DOI: 10.1016/S0140-6736(16)31803-7
Comparison of stapled haemorrhoidopexy with traditional excisional surgery for haemorrhoidal disease (eTHoS): a pragmatic, multicentre, randomised controlled trial
Erratum in
-
Department of Error.Lancet. 2016 Nov 12;388(10058):2354. doi: 10.1016/S0140-6736(16)32059-1. Epub 2016 Oct 26. Lancet. 2016. PMID: 35395707 Free PMC article. No abstract available.
Abstract
Background: Two commonly performed surgical interventions are available for severe (grade II-IV) haemorrhoids; traditional excisional surgery and stapled haemorrhoidopexy. Uncertainty exists as to which is most effective. The eTHoS trial was designed to establish the clinical effectiveness and cost-effectiveness of stapled haemorrhoidopexy compared with traditional excisional surgery.
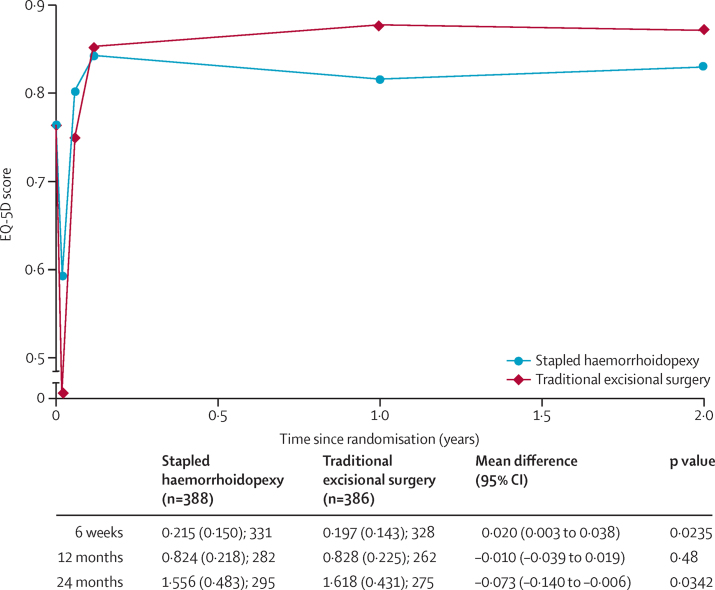
Methods: The eTHoS trial was a large, open-label, multicentre, parallel-group, pragmatic randomised controlled trial done in adult participants (aged 18 years or older) referred to hospital for surgical treatment for grade II-IV haemorrhoids. Participants were randomly assigned (1:1) to receive either traditional excisional surgery or stapled haemorrhoidopexy. Randomisation was minimised according to baseline EuroQol 5 dimensions 3 level score (EQ-5D-3L), haemorrhoid grade, sex, and centre with an automated system to stapled haemorrhoidopexy or traditional excisional surgery. The primary outcome was area under the quality of life curve (AUC) measured with the EQ-5D-3L descriptive system over 24 months, assessed according to the randomised groups. The primary outcome measure was analysed using linear regression with adjustment for the minimisation variables. This trial is registered with the ISRCTN registry, number ISRCTN80061723.
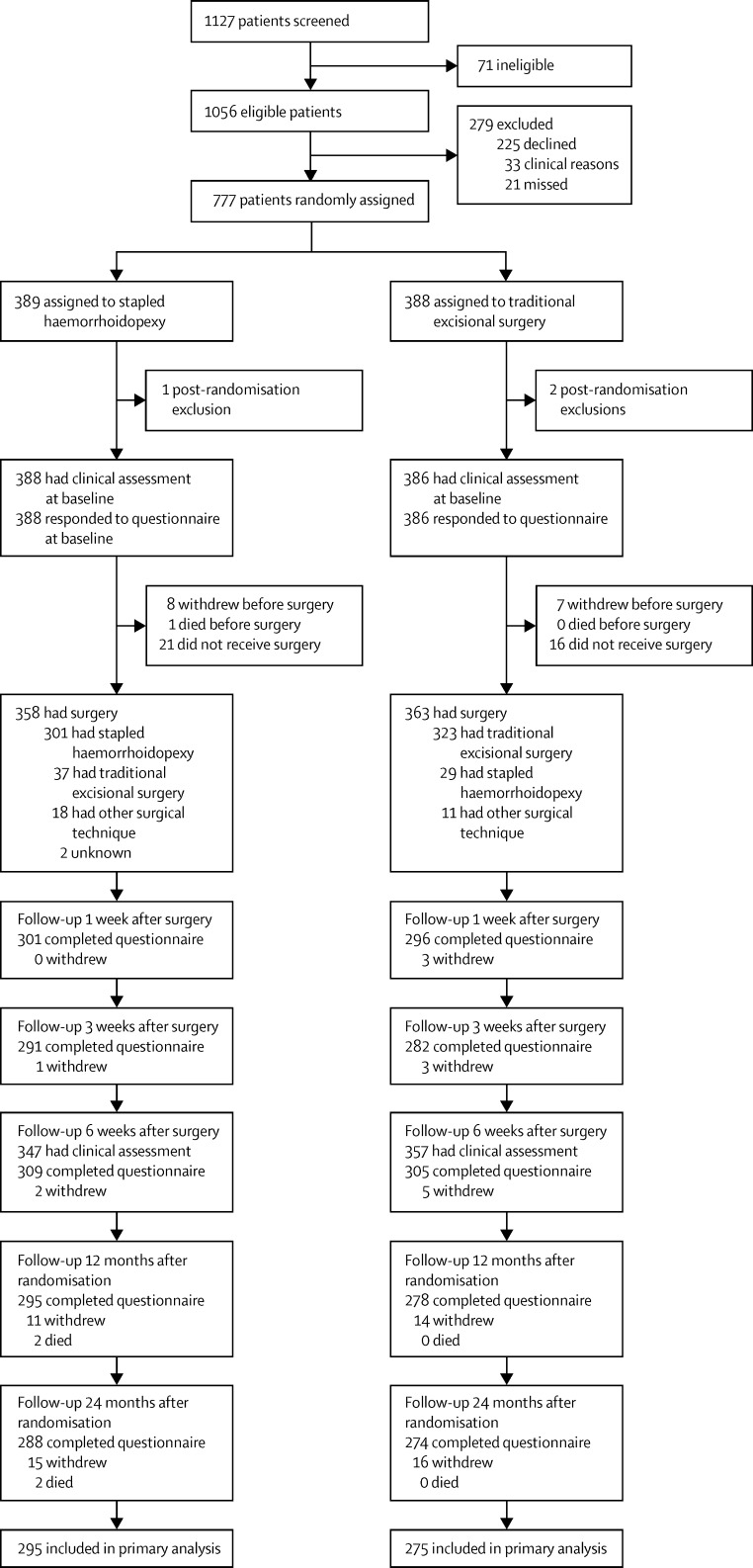
Findings: Between Jan 13, 2011, and Aug 1, 2014, 777 patients were randomised (389 to receive stapled haemorrhoidopexy and 388 to receive traditional excisional surgery). Stapled haemorrhoidopexy was less painful than traditional excisional surgery in the short term and surgical complication rates were similar between groups. The EQ-5D-3L AUC score was higher in the traditional excisional surgery group than the stapled haemorrhoidopexy group over 24 months; mean difference -0·073 (95% CI -0·140 to -0·006; p=0·0342). EQ-5D-3L was higher for stapled haemorrhoidopexy in the first 6 weeks after surgery, the traditional excisional surgery group had significantly better quality of life scores than the stapled haemorrhoidopexy group. 24 (7%) of 338 participants who received stapled haemorrhoidopexy and 33 (9%) of 352 participants who received traditional excisional surgery had serious adverse events.
Interpretation: As part of a tailored management plan for haemorrhoids, traditional excisional surgery should be considered over stapled haemorrhoidopexy as the surgical treatment of choice.
Funding: National Institute for Health Research Health Technology Assessment programme.
Copyright © 2016 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
eTHoS piles pressure on haemorrhoidopexy.Lancet. 2016 Nov 12;388(10058):2328-2330. doi: 10.1016/S0140-6736(16)31802-5. Epub 2016 Oct 7. Lancet. 2016. PMID: 27726952 No abstract available.
References
-
- Riss S, Weiser FA, Schwameis K. The prevalence of hemorrhoids in adults. Int J Colorectal Dis. 2012;27:215–220. - PubMed
-
- Johanson JF, Sonnenberg A. The prevalence of hemorrhoids and chronic constipation. An epidemiologic study. Gastroenterology. 1990;98:380–386. - PubMed
-
- Goligher JC. Surgery of the anus, rectum, and colon. 5th edn. Bailliere Tindall; London: 1984. pp. 993–996.
-
- NHS IC. Hospital episode statistics (procedure search). 2004–05. http://www.hesonline.nhs.uk/Ease/servlet/ContentServer?siteID=1937&categ... (accessed July 31, 2016).
-
- Lacerda-Filho A, Da Silva RG. Stapled hemorrhoidectomy: present status. Arq Gastroenterol. 2005;42:191–194. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
