

The Intensity of Primary Care for Heart Failure Patients: A Determinant of Readmissions? The CarPaths Study: A French Region-Wide Analysis
- PMID: 27727296
- PMCID: PMC5058477
- DOI: 10.1371/journal.pone.0163268
The Intensity of Primary Care for Heart Failure Patients: A Determinant of Readmissions? The CarPaths Study: A French Region-Wide Analysis
Abstract
Background: We aimed to classify patients with heart failure (HF) by the style of primary care they receive.
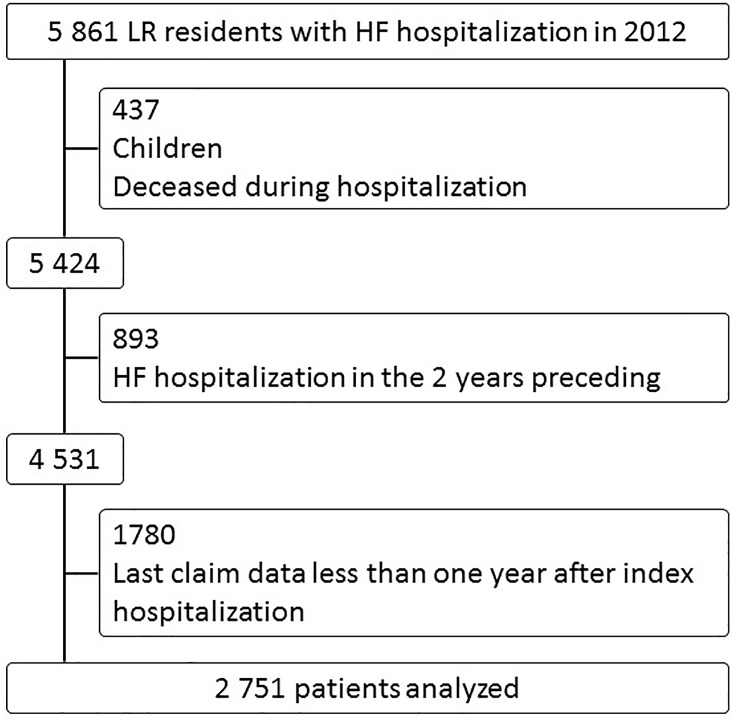
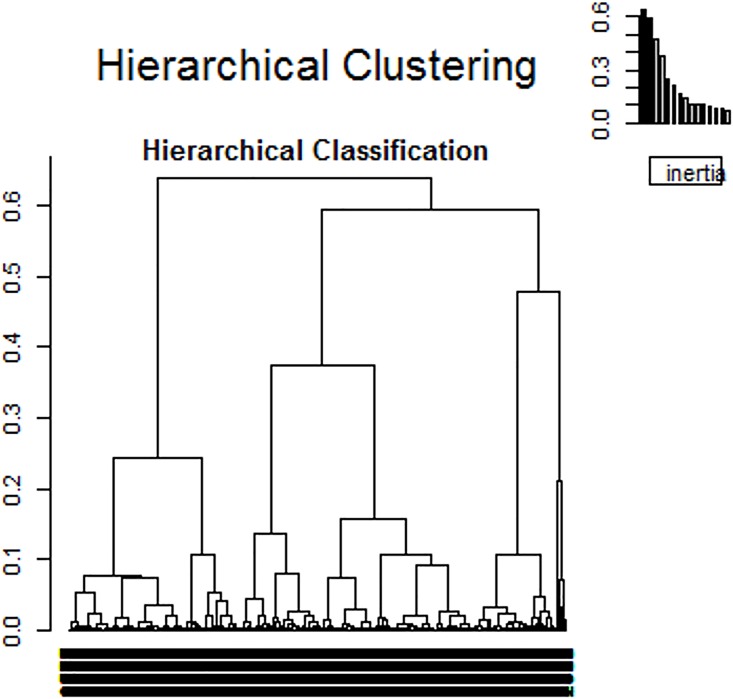
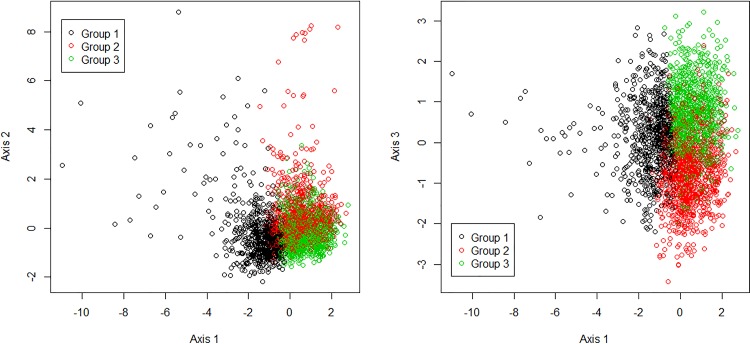
Methods and results: We used the claim data (SNIIRAM: Système National d'Information Inter-Régime de l'Assurance Maladie) of patients living in a French region. We evaluated three concepts. First, baseline clinical status with age and Charlson index. Second, primary care practice style with mean delay between consultations, quantity of nursing care, and variability of diuretic dose. Third, clinical outcomes with death during follow-up, readmission for HF, and rate of unforeseen consultations. The baseline clinical status and the clinical outcomes were included to give an insight in the reasons for, and performance of, primary care practice style. Patients were classified using a hierarchical ascending classification based on principal components. A total of 2,751 patients were included in this study and were followed for a median of 22 months. The mean age was 78 y (SD: 12); 484 (18%) died, and 818 (30%) were readmitted for HF. We found three different significant groups characterized by their need for care and the intensity of practice style: group 1 (N = 734) was "low need-low intensity"; group 2 (N = 1,060) was "high need-low intensity"; and group 3 (N = 957) was "high need-high intensity". Their readmission rates were 17%, 41% and 28%, respectively.
Conclusions: This study evaluated the link between primary care, clinical status and main clinical outcomes in HF patients. In higher need patients, a low-intensity practice style was associated with poorer clinical outcomes.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Capomolla S, Febo O, Ceresa M, Caporotondi A, Guazzotti G, La Rovere MT, et al. Cost/utility ratio in chronic heart failure: comparison between heart failure management program delivered by day-hospital and usual care. J Am Coll Cardiol. 2002;40: 1259–1266. 10.1016/s0735-1097(02)02140-x - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
