

Defining response to radiotherapy in rectal cancer using magnetic resonance imaging and histopathological scales
- PMID: 27729748
- PMCID: PMC5055872
- DOI: 10.3748/wjg.v22.i37.8414
Defining response to radiotherapy in rectal cancer using magnetic resonance imaging and histopathological scales
Abstract
Aim: To define good and poor regression using pathology and magnetic resonance imaging (MRI) regression scales after neo-adjuvant chemotherapy for rectal cancer.
Methods: A systematic review was performed on all studies up to December 2015, without language restriction, that were identified from MEDLINE, Cochrane Controlled Trials Register (1960-2015), and EMBASE (1991-2015). Searches were performed of article bibliographies and conference abstracts. MeSH and text words used included "tumour regression", "mrTRG", "poor response" and "colorectal cancers". Clinical studies using either MRI or histopathological tumour regression grade (TRG) scales to define good and poor responders were included in relation to outcomes [local recurrence (LR), distant recurrence (DR), disease-free survival (DFS), and overall survival (OS)]. There was no age restriction or stage of cancer restriction for patient inclusion. Data were extracted by two authors working independently and using pre-defined outcome measures.
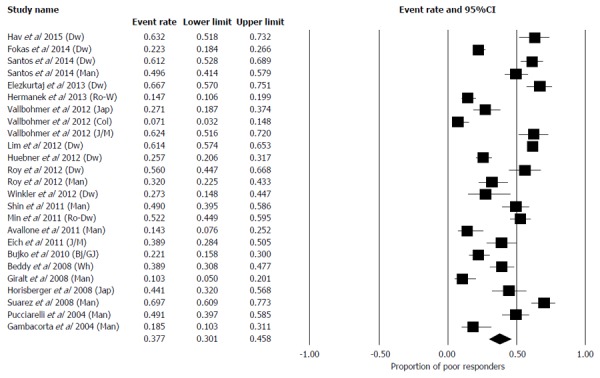
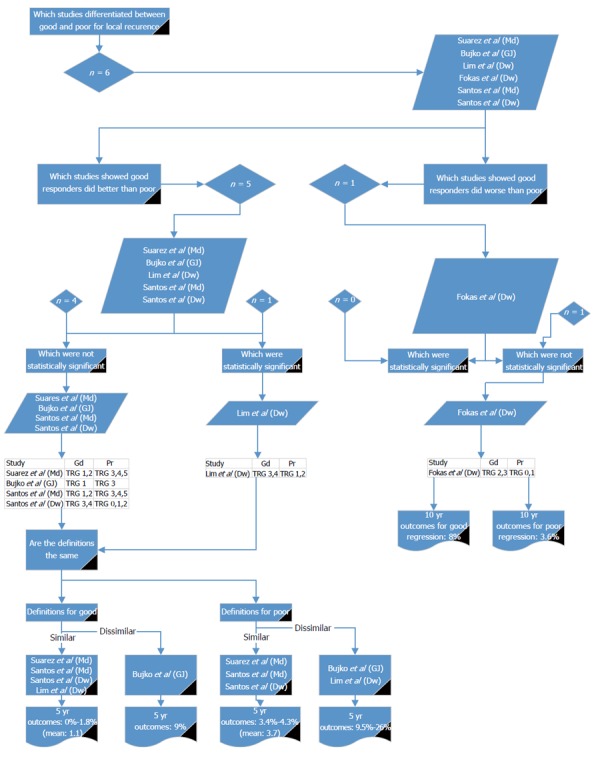
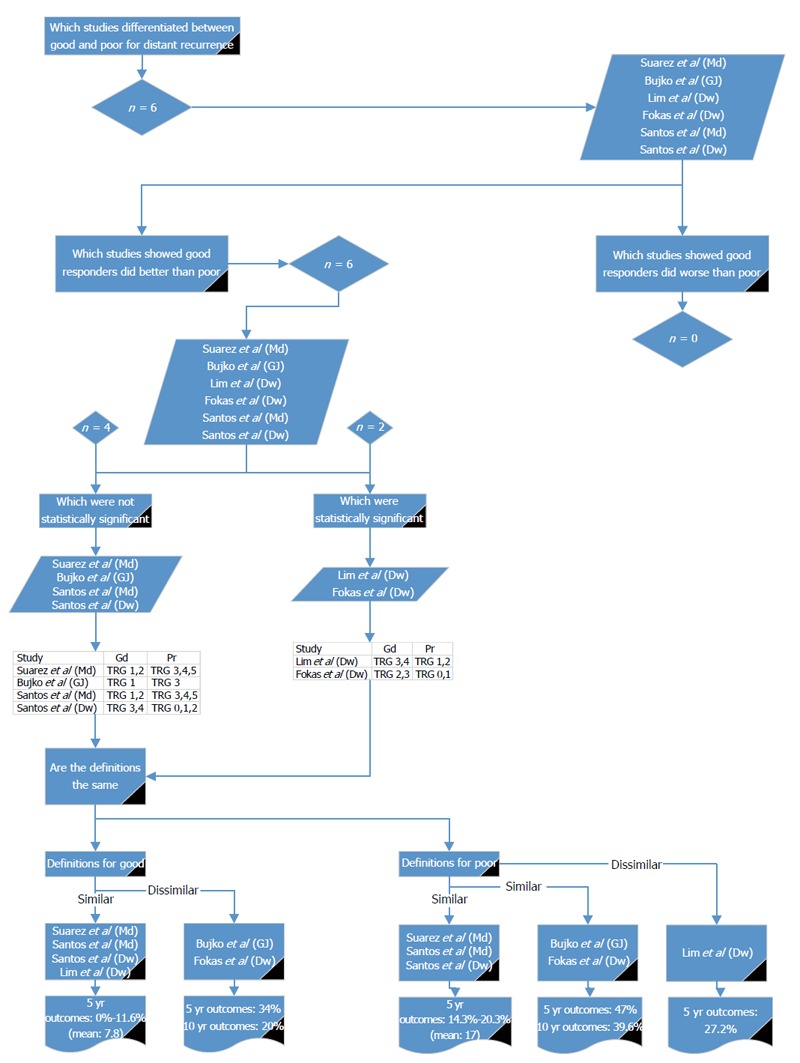
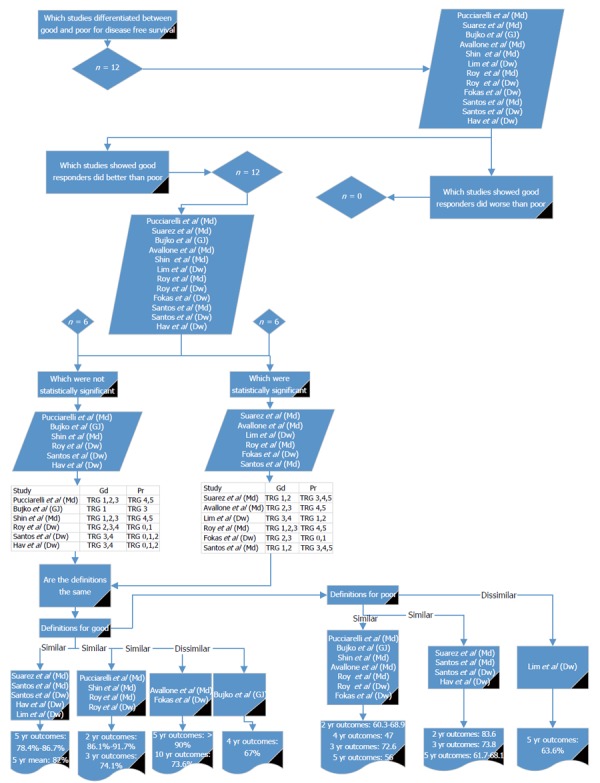
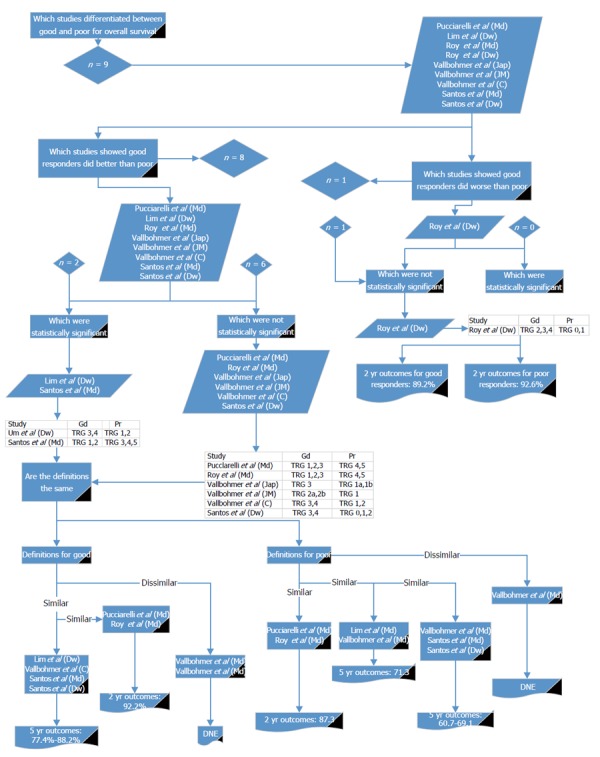
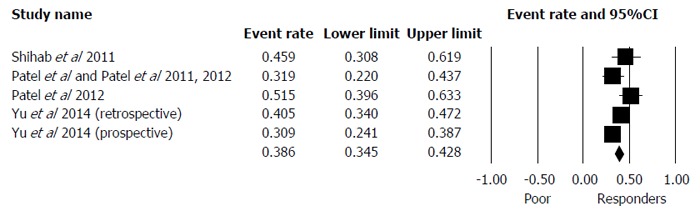
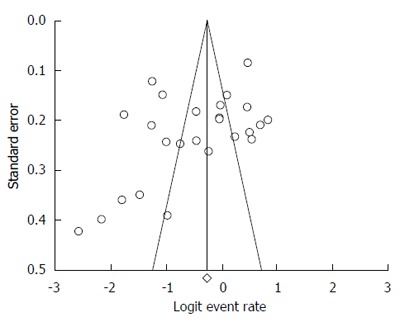
Results: Quantitative data (prevalence) were extracted and analysed according to meta-analytical techniques using comprehensive meta-analysis. Qualitative data (LR, DR, DFS and OS) were presented as ranges. The overall proportion of poor responders after neo-adjuvant chemo-radiotherapy (CRT) was 37.7% (95%CI: 30.1-45.8). There were 19 different reported histopathological scales and one MRI regression scale (mrTRG). Clinical studies used nine and six histopathological scales for poor and good responders, respectively. All studies using MRI to define good and poor response used one scale. The most common histopathological definition for good response was the Mandard grades 1 and 2 or Dworak grades 3 and 4; Mandard 3, 4 and 5 and Dworak 0, 1 and 2 were used for poor response. For histopathological grades, the 5-year outcomes for poor responders were LR 3.4%-4.3%, DR 14.3%-20.3%, DFS 61.7%-68.1% and OS 60.7-69.1. Good pathological response 5-year outcomes were LR 0%-1.8%, DR 0%-11.6%, DFS 78.4%-86.7%, and OS 77.4%-88.2%. A poor response on MRI (mrTRG 4,5) resulted in 5-year LR 4%-29%, DR 9%, DFS 31%-59% and OS 27%-68%. The 5-year outcomes with a good response on MRI (mrTRG 1,2 and 3) were LR 1%-14%, DR 3%, DFS 64%-83% and OS 72%-90%.
Conclusion: For histopathology regression assessment, Mandard 1, 2/Dworak 3, 4 should be used for good response and Mandard 3, 4, 5/Dworak 0, 1, 2 for poor response. MRI indicates good and poor response by mrTRG1-3 and mrTRG4-5, respectively.
Keywords: Neo-adjuvant therapy; Poor response; Rectal cancer; Tumour regression; mrTRG.
Conflict of interest statement
Conflict-of-interest statement: None to declare.
Figures
References
-
- MacGregor TP, Maughan TS, Sharma RA. Pathological grading of regression following neoadjuvant chemoradiation therapy: the clinical need is now. J Clin Pathol. 2012;65:867–871. - PubMed
-
- Chua YJ, Barbachano Y, Cunningham D, Oates JR, Brown G, Wotherspoon A, Tait D, Massey A, Tebbutt NC, Chau I. Neoadjuvant capecitabine and oxaliplatin before chemoradiotherapy and total mesorectal excision in MRI-defined poor-risk rectal cancer: a phase 2 trial. Lancet Oncol. 2010;11:241–248. - PubMed
-
- Marijnen CA, Glimelius B. The role of radiotherapy in rectal cancer. Eur J Cancer. 2002;38:943–952. - PubMed
-
- Påhlman L, Hohenberger W, Günther K, Fietkau R, Metzger U. Is radiochemotherapy necessary in the treatment of rectal cancer? Eur J Cancer. 1998;34:438–448. - PubMed
-
- Patel UB, Blomqvist LK, Taylor F, George C, Guthrie A, Bees N, Brown G. MRI after treatment of locally advanced rectal cancer: how to report tumor response--the MERCURY experience. AJR Am J Roentgenol. 2012;199:W486–W495. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
