

Risk Stratification in Lung Resection
- PMID: 27730011
- PMCID: PMC5030224
- DOI: 10.1007/s40137-016-0158-x
Risk Stratification in Lung Resection
Abstract
Purpose of review: Surgery is considered the best treatment option for patients with early stage lung cancer. Nevertheless, lung resection may cause a variable functional impairment that could influence the whole cardio-respiratory system with potential life-threatening complications. The aim of the present study is to review the most relevant evidences about the evaluation of surgical risk before lung resection, in order to define a practical approach for the preoperative functional assessment in lung cancer patients.
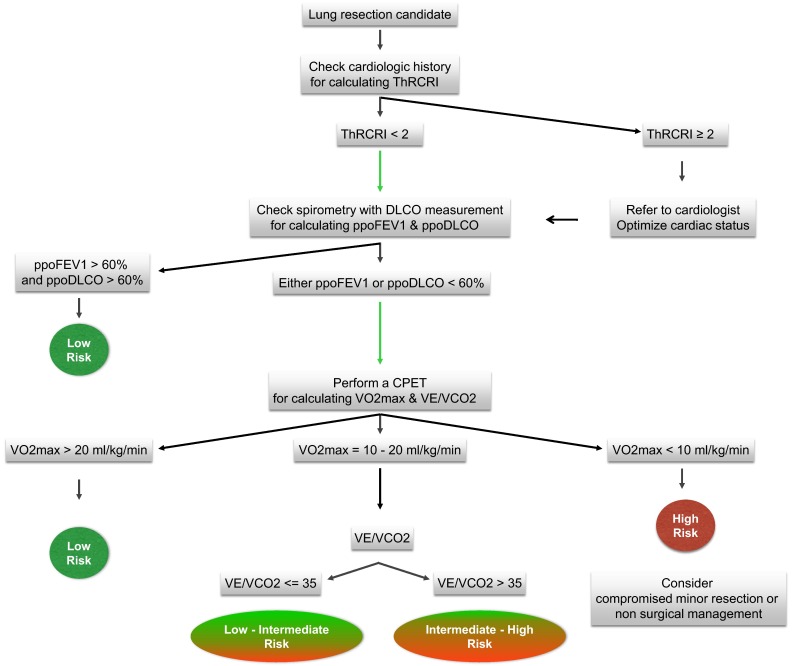
Recent findings: The first step in the preoperative functional evaluation of a lung resection candidate is a cardiac risk assessment. The predicted postoperative values of forced expiratory volume in one second and carbon monoxide lung diffusion capacity should be estimated next. If both values are greater than 60 % of the predicted values, the patients are regarded to be at low surgical risk. If either or both of them result in values lower than 60 %, then a cardiopulmonary exercise test is recommended. Patients with VO2max >20 mL/kg/min are regarded to be at low risk, while those with VO2max <10 mL/kg/min at high risk. Values of VO2max between 10 and 20 mL/kg/min require further risk stratification by the VE/VCO2 slope. A VE/VCO2 <35 indicates an intermediate-low risk, while values above 35 an intermediate-high risk.
Summary: The recent scientific evidence confirms that the cardiologic evaluation, the pulmonary function test with DLCO measurement, and the cardiopulmonary exercise test are the cornerstones of the preoperative functional evaluation before lung resection. We present a simplified functional algorithm for the surgical risk stratification in lung resection candidates.
Keywords: Cardiac risk; Co-morbidities; Exercise test; Lung cancer surgery; Lung resection; Morbidity; Mortality; Operative Risk; Preoperative evaluation; Pulmonary function.
Conflict of interest statement
Compliance with Ethics Guidelines Conflict of Interest Dr. Brunelli reports personal fees from Bard Davol Inc. Dr. Salati declares no conflicts of interest relevant to this manuscript. Human and Animal Rights and Informed Consent This article does not contain any studies with human or animal subjects performed by any of the authors.
Figures
References
-
- •• Brunelli A, Kim AW, Berger KI, Addrizzo-Harris DJ. Physiologic evaluation of the patient with lung cancer being considered for resectional surgery. Chest 2013;143:166S–190S. The Authors performed a rigorous review of the medical literature proposing a list of evidence based recommendations and an exhaustive algorithm for the preoperative physiologic assessment in patients candidates to lung resection for NSCLC. Once performed the cardiac and spirometric evaluations with the estimation of the FEV1 and DLCO predictive postoperative values, the final risk stratification should be obtained considering the VO2max measured at the cardiopulmonary exercise test.
-
- Brunelli A, Charloux A, Bolliger CT, Rocco G, Sculier JP, Varela G, Licker M, Ferguson MK, Faivre-Finn C, Huber RM, Clini EM, Win T, De Ruysscher D, European Respiratory Society and European Society of Thoracic Surgeons joint task force on fitness for radical therapy ERS/ESTS clinical guidelines on fitness for radical therapy in lung cancer patients (surgery and chemo-radiotherapy) Eur Respir J. 2009;34:17–41. doi: 10.1183/09031936.00184308. - DOI - PubMed
-
- Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, Cook EF, Sugarbaker DJ, Donaldson MC, Poss R, Ho KK, Ludwig LE, Pedan A, Goldman L. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation. 1999;100:1043–1049. doi: 10.1161/01.CIR.100.10.1043. - DOI - PubMed
-
- • Brunelli A, Cassivi SD, Fibla J, Halgren LA, Wigle DA, Allen MS, Nichols FC, Shen KR, Deschamps C. External validation of the recalibrated thoracic revised cardiac risk index for predicting the risk of major cardiac complications after lung resection. Ann Thorac Surg. 2011;92:445–448. The Authors validated the use of a multiparametric cardiac risk index (ThRCRI) developed to assess the risk of adverse cardiac events after lung resection. They found, in a cohort of 2,621 patients, a progressive increase of observed complication rate in line with the class of risk assigned to the patients (class A: cardiac complication rate 0.9%, B: 4.2%, C: 8%, D: 18%). This study confirm the reliability of the ThRCRI. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials