

Patterns, predictors and outcomes of asthma control and exacerbations during pregnancy: a prospective cohort study
- PMID: 27730170
- PMCID: PMC5005153
- DOI: 10.1183/23120541.00054-2015
Patterns, predictors and outcomes of asthma control and exacerbations during pregnancy: a prospective cohort study
Abstract
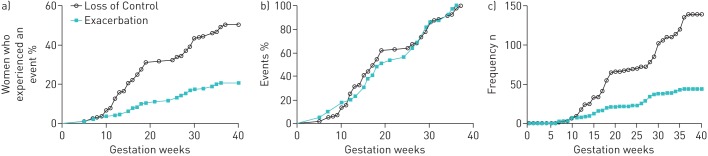
There exists a paucity of data for socially disadvantaged populations describing patterns and predictors of asthma control status and exacerbations during pregnancy, and their relationship to adverse perinatal outcomes. Asthmatic women (n=189) were followed prospectively during pregnancy, with visits at 12, 20, 28 and 36 weeks gestation. Data on loss of control, recurrent uncontrolled asthma and moderate/severe exacerbations were collected at each visit and their relationship to perinatal outcomes examined following stratification for fetal sex. 50% of asthmatic women experienced a loss of control or moderate/severe exacerbation during pregnancy, with 22% of women experiencing a moderate/severe exacerbation. Factors associated with an increased risk of women experiencing recurrent uncontrolled asthma during pregnancy included smoking (relative risk 2.92, 95% CI 1.53-5.58), inhaled corticosteroid use at the beginning of pregnancy (relative risk 2.40, 95% CI 1.25-4.60) and increasing maternal age (relative risk 1.06, 95% CI 1.01-1.11). No factors were associated with moderate/severe exacerbations. Asthma control rather than exacerbations during pregnancy appeared to be most strongly correlated with perinatal outcomes. Following stratification by fetal sex, the presence of recurrent uncontrolled asthma was associated with an increased risk of being small for gestational age in women pregnant with females (33.3% versus 9.5%; p=0.018). In contrast, there was a nonsignificant increased risk of preterm birth in women with recurrent uncontrolled asthma that were pregnant with males (25.0% versus 11.8%; p=0.201) These results suggest that the key to improving perinatal outcomes lies in improving asthma control as early as possible in pregnancy and monitoring throughout pregnancy, rather than focusing on preventing exacerbations alone.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Bracken MB, Triche EW, Belanger K, et al. Asthma symptoms, severity, and drug therapy: a prospective study of effects on 2205 pregnancies. Obstet Gynecol 2003; 102: 739–752. - PubMed
-
- Schatz M. Asthma during pregnancy: interrelationships and management. Ann Allergy 1992; 68: 123–133. - PubMed
-
- Schatz M, Dombrowski MP, Wise R, et al. Asthma morbidity during pregnancy can be predicted by severity classification. J Allergy Clin Immunol 2003; 112: 283–288. - PubMed
-
- Murphy VE, Gibson PG, Smith R, et al. Asthma during pregnancy: mechanisms and treatment implications. Eur Respir J 2005; 25: 731–750. - PubMed
-
- Murphy VE, Gibson P, Talbot PI, et al. Severe asthma exacerbations during pregnancy. Obstet Gynecol 2005; 106: 1046–1054. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources