

Long-Term Prediction of the Demand of Colonoscopies Generated by a Population-Based Colorectal Cancer Screening Program
- PMID: 27732635
- PMCID: PMC5061389
- DOI: 10.1371/journal.pone.0164666
Long-Term Prediction of the Demand of Colonoscopies Generated by a Population-Based Colorectal Cancer Screening Program
Abstract
Objective: To estimate the long-term need for colonoscopies after a positive fecal immunochemical test (FIT) and post-polypectomy surveillance in the context of a population-based colorectal cancer (CRC) screening program.
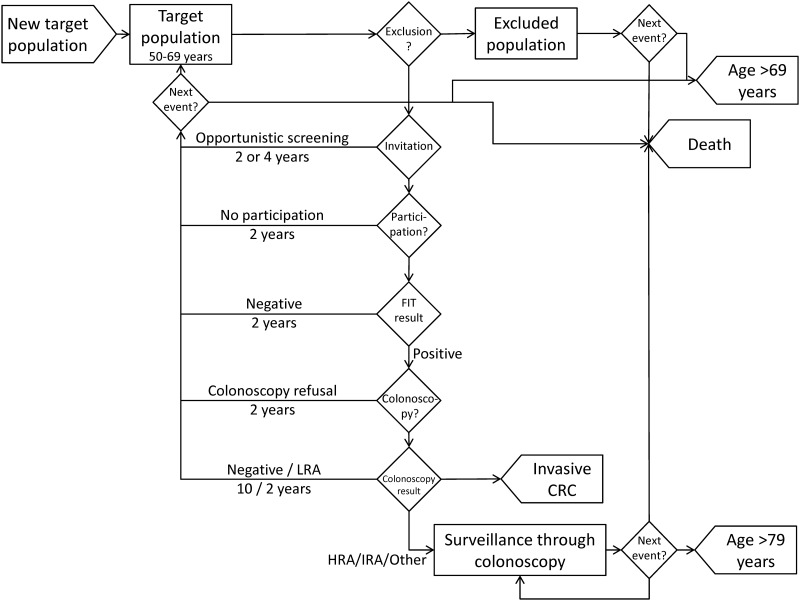
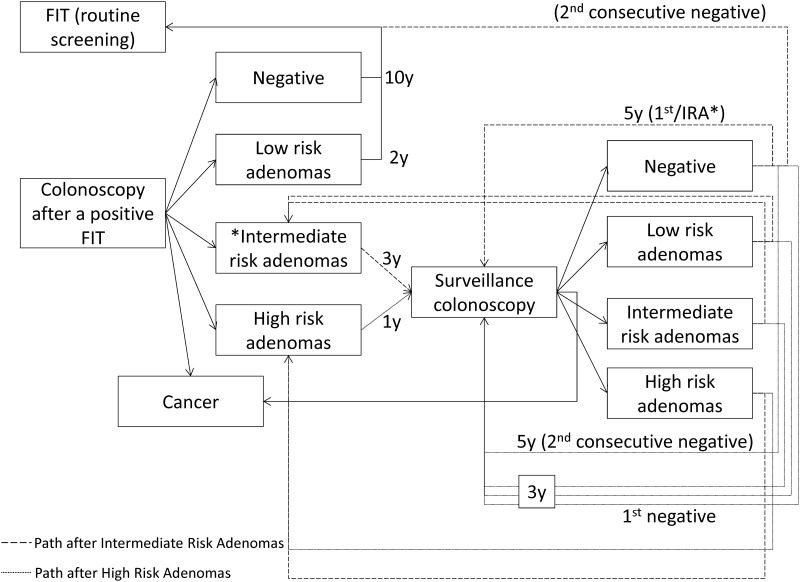
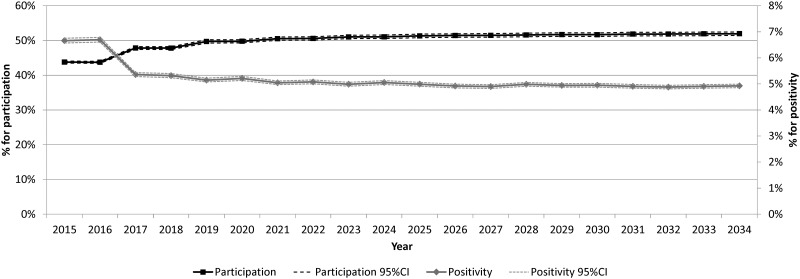
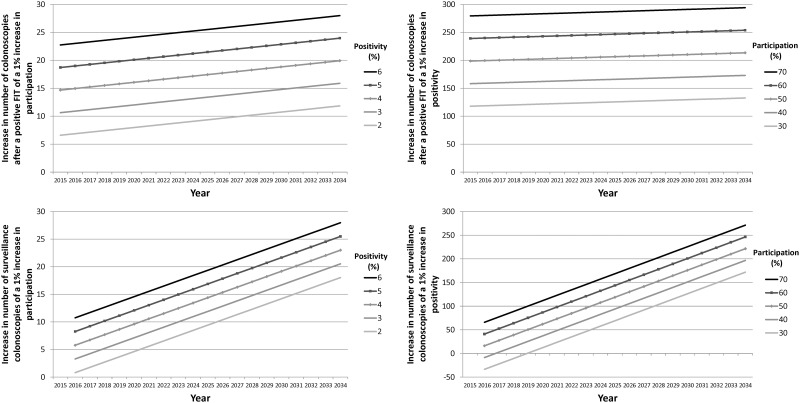
Methods: A discrete-event simulation model was built to reproduce the process of CRC screening and post-polypectomy surveillance following European guidelines in a population of 100,000 men and women aged 50-69 years over a 20-year period. Screening consisted of biennial FIT and colonoscopy in participants with positive results. The model was mainly fed using data from the first and second rounds of a Spanish program (2010-2013). Data on post-polypectomy surveillance results were obtained from the literature. A probabilistic multivariate sensitivity analysis was performed on the effect of participation, FIT positivity, and adherence to surveillance colonoscopies. The main outcome variables were the number of colonoscopies after a positive FIT, surveillance colonoscopies, and the overall number of colonoscopies.
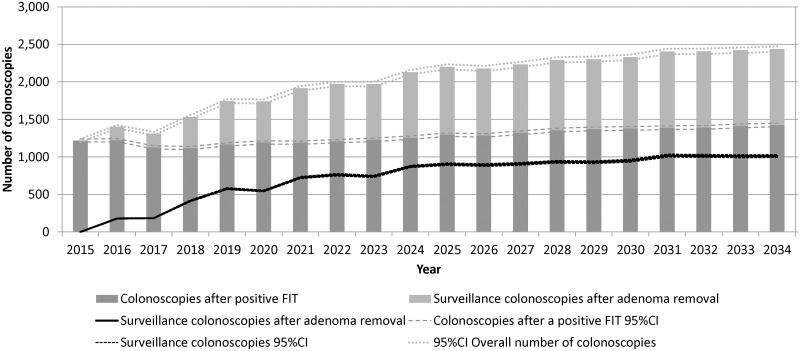
Results: An average yearly number of 1,200 colonoscopies after a positive FIT were predicted per 100,000 inhabitants with a slight increase to 1,400 at the end of the 20-year period. Surveillance colonoscopies increased to an average of 1,000 per 100,000 inhabitants in the long-term, showing certain stabilization in the last years of the 20-year simulation horizon. The results were highly sensitive to FIT positivity.
Conclusions: Implementing a population-based CRC screening program will increase the demand for colonoscopies, which is expected to double in 20 years, mainly due to an increase in surveillance colonoscopies.
Conflict of interest statement
Author JM received funding from Roche Diagnostics International Ltd., a commercial company, for this study. There are no patents, products in development or marketed products to declare. This does not alter our adherence to all the PLOS ONE policies on sharing data and materials.
Figures
References
-
- European Commission. European Guidelines for quality assurance in colorectal cancer screening and diagnosis. 2010. Available: http://bookshop.europa.eu/en/european-guidelines-for-quality-assurance-i....
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
