

Cortical bone deficit and fat infiltration of bone marrow and skeletal muscle in ambulatory children with mild spastic cerebral palsy
- PMID: 27732905
- PMCID: PMC5912954
- DOI: 10.1016/j.bone.2016.10.005
Cortical bone deficit and fat infiltration of bone marrow and skeletal muscle in ambulatory children with mild spastic cerebral palsy
Abstract
Introduction: Nonambulatory children with severe cerebral palsy (CP) have underdeveloped bone architecture, low bone strength and a high degree of fat infiltration in the lower extremity musculature. The present study aims to determine if such a profile exists in ambulatory children with mild CP and if excess fat infiltration extends into the bone marrow.
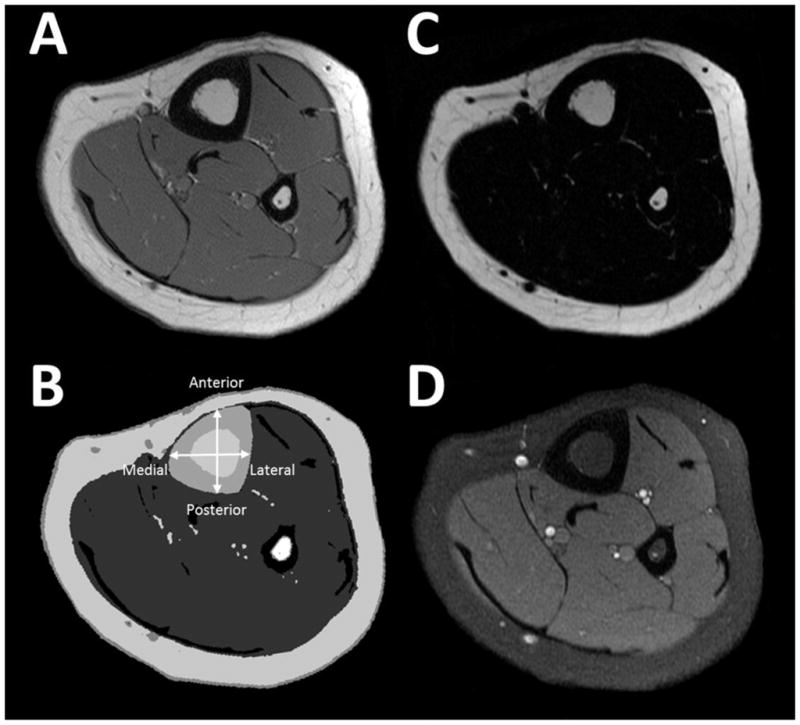
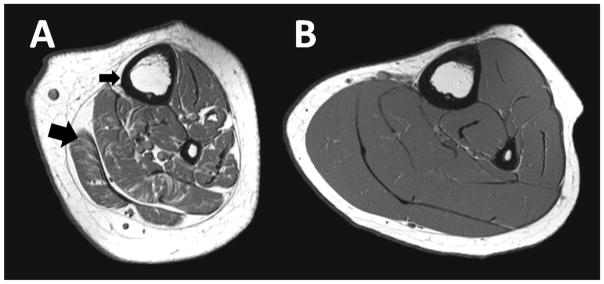
Materials and methods: Ambulatory children with mild spastic CP and typically developing children (4 to 11years; 12/group) were compared. Magnetic resonance imaging was used to estimate cortical bone, bone marrow and total bone volume and width, bone strength [i.e., section modulus (Z) and polar moment of inertia (J)], and bone marrow fat concentration in the midtibia, and muscle volume, intermuscular, subfascial, and subcutaneous adipose tissue (AT) volume and intramuscular fat concentration in the midleg. Accelerometer-based activity monitors worn on the ankle were used to assess physical activity.
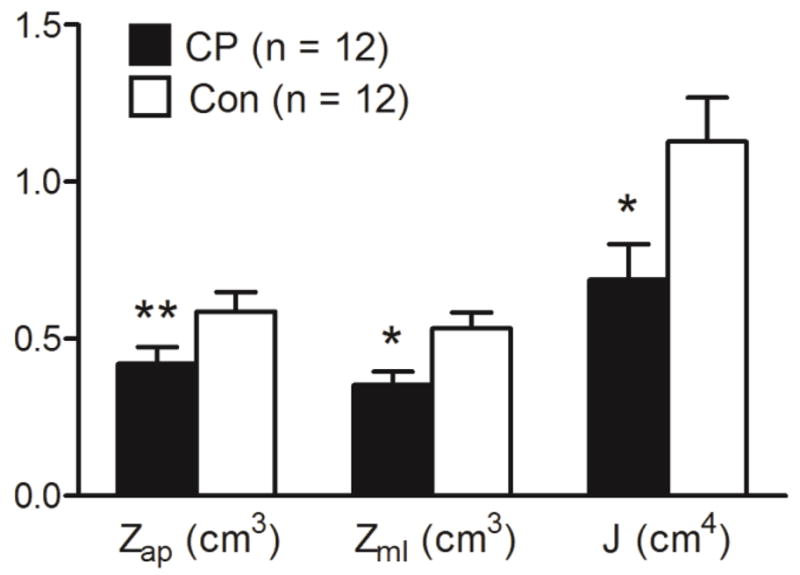
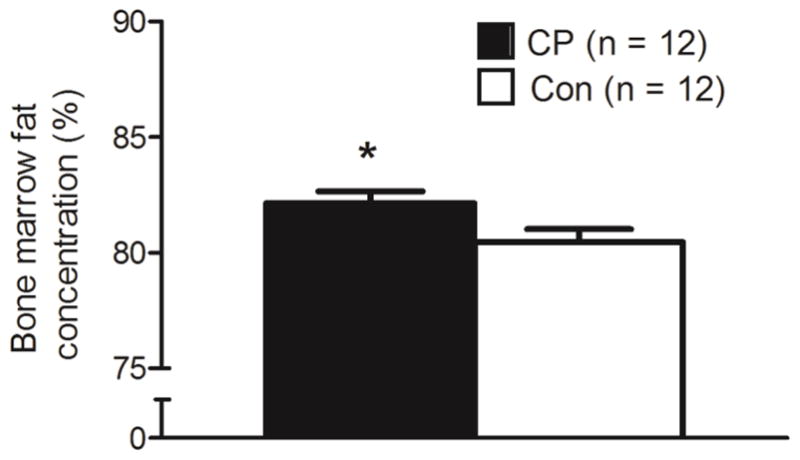
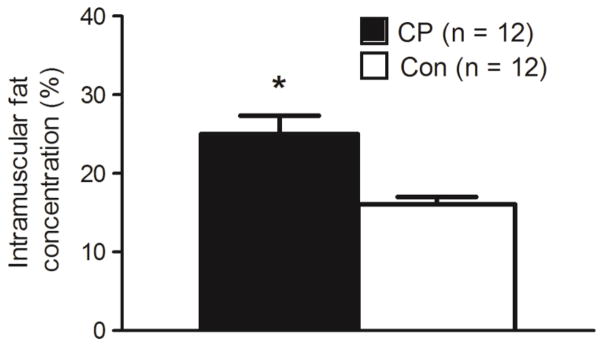
Results: There were no group differences in age, height, body mass, body mass percentile, BMI, BMI percentile or tibia length, but children with CP had lower height percentile (19th vs. 50th percentile) and total physical activity counts (44%) than controls (both p<0.05). Children with CP also had lower cortical bone volume (30%), cortical bone width in the posterior (16%) and medial (32%) portions of the shaft, total bone width in the medial-lateral direction (15%), Z in the medial-lateral direction (34%), J (39%) and muscle volume (39%), and higher bone marrow fat concentration (82.1±1.8% vs. 80.5±1.9%), subfascial AT volume (3.3 fold) and intramuscular fat concentration (25.0±8.0% vs. 16.1±3.3%) than controls (all p<0.05). When tibia length was statistically controlled, all group differences in bone architecture, bone strength, muscle volume and fat infiltration estimates, except posterior cortical bone width, were still present (all p<0.05). Furthermore, a higher intermuscular AT volume in children with CP compared to controls emerged (p<0.05).
Conclusions: Ambulatory children with mild spastic CP exhibit an underdeveloped bone architecture and low bone strength in the midtibia and a greater infiltration of fat in the bone marrow and surrounding musculature compared to typically developing children. Whether the deficit in the musculoskeletal system of children with CP is associated with higher chronic disease risk and whether the deficit can be mitigated requires further investigation.
Keywords: Bone strength; Bone structure; Cerebral palsy; Fat depots; Unloading.
Copyright © 2016 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of Interest: Daniel G. Whitney, Harshvardhan Singh, Freeman Miller, Mary F. Barbe, Jill M. Slade and Christopher M. Modlesky declare that they have no conflicts of interest.
Figures
References
-
- Morgan P, McGinley J. Gait function and decline in adults with cerebral palsy: a systematic review. Disabil Rehabil. 2014;36:1–9. - PubMed
-
- Modlesky CM, Whitney DG, Singh H, Barbe MF, Kirby JT, Miller F. Underdevelopment of trabecular bone microarchitecture in the distal femur of nonambulatory children with cerebral palsy becomes more pronounced with distance from the growth plate. Osteoporos Int. 2015;26:505–12. - PubMed
-
- Modlesky CM, Subramanian P, Miller F. Underdeveloped trabecular bone microarchitecture is detected in children with cerebral palsy using high-resolution magnetic resonance imaging. Osteoporos Int. 2008;19:169–76. - PubMed
-
- Henderson RC, Lark RK, Gurka MJ, Worley G, Fung EB, Conaway M, Stallings VA, Stevenson RD. Bone density and metabolism in children and adolescents with moderate to severe cerebral palsy. Pediatrics. 2002;110:e5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
