

Establishment of the Human Uteroplacental Circulation: A Historical Perspective
- PMID: 27733657
- PMCID: PMC5933180
- DOI: 10.1177/1933719116669056
Establishment of the Human Uteroplacental Circulation: A Historical Perspective
Abstract
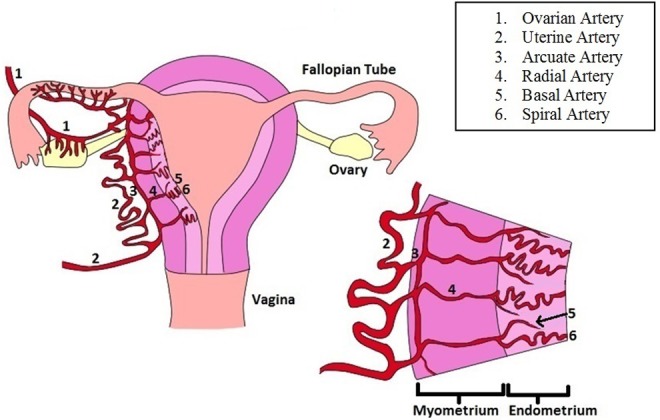
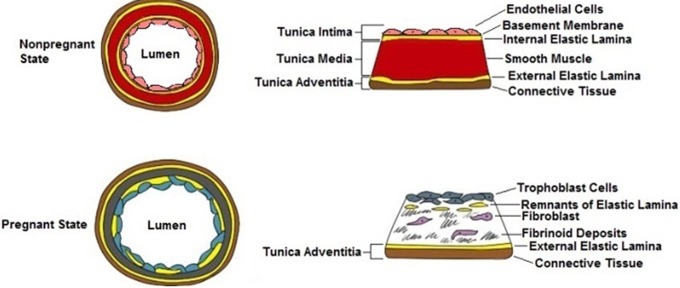
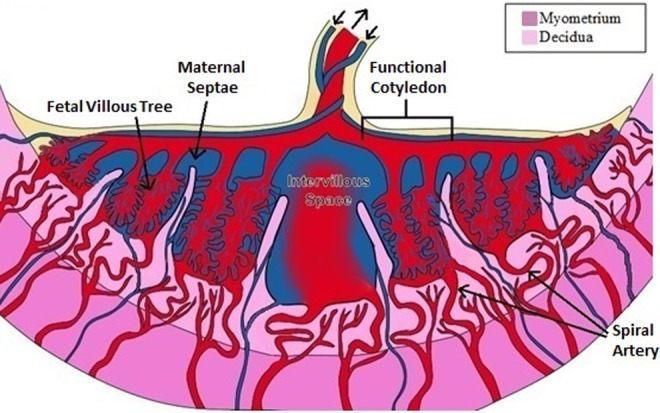
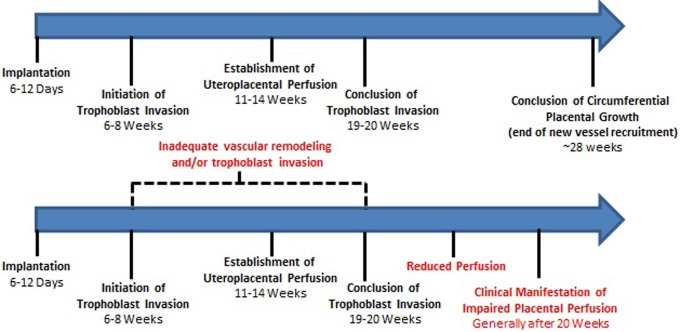
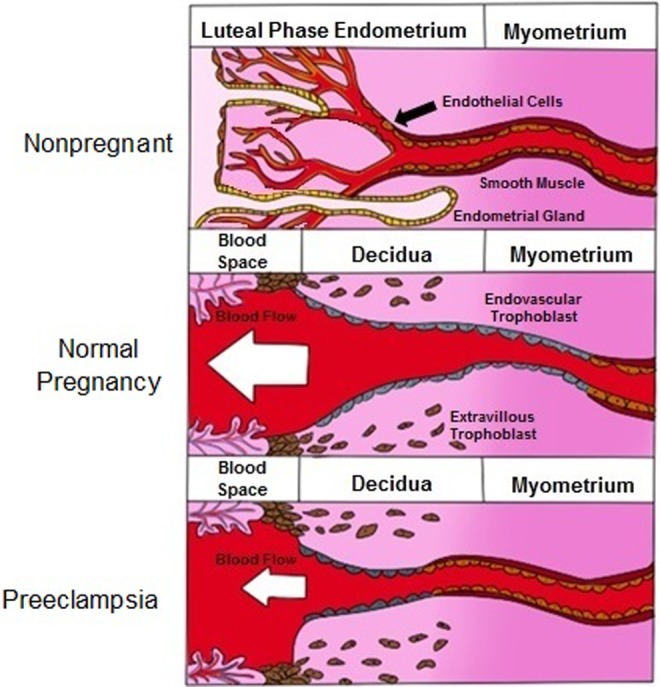
The uterine vasculature undergoes marked changes during pregnancy in order to provide the necessary increase in blood flow to support growth and nutrition of the uterus, placenta, and developing fetus. Pregnancy-associated uterine vascular transformations are orchestrated by a complex array of endocrine and cellular mechanisms to bring about structural modifications at the maternal-fetal interface, which collectively lead to development of the uteroplacental circulation. Understanding intrinsic uterine vascular remodeling in pregnancy is essential for understanding the physiologic and pathophysiologic regulation of maternal uterine blood flow. Aberrations of uterine vascular remodeling are potentially involved in the etiology of several pregnancy disorders, for example, preeclampsia, fetal growth restriction, and preterm labor; therefore, it is essential for subspecialist clinicians and investigators interested in reproductive physiology to fully understand the establishment of uteroplacental circulation. The foundational literature in this area is extensive; thus, a succinct review is likely to be a useful resource. Herein, we present and discuss a historical perspective on uterine vascular anatomy, maternal vascular growth associated with decidualization, trophoblast invasion, intervillous circulation, aberrations in uterine vascular modeling, and the clinical implications of improper development of the uteroplacental circulation.
Keywords: placenta; preeclampsia; pregnancy complications.
Conflict of interest statement
Figures
References
-
- Intengan HD, Schiffrin EL. Vascular remodeling in hypertension: roles of apoptosis, inflammation, and fibrosis. Hypertension.2001;38(3 pt 2):581–587. - PubMed
-
- Mulvany MJ. Vascular remodelling of resistance vessels: can we define this? Cardiovasc Res. 1999;41(1):9–13. - PubMed
-
- Dixon HG, Robertson WB. A study of the vessels of the placental bed in normotensive and hypertensive women. J Obstet Gynaecol Br Emp. 1958;65(5):803–809. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
