

Chest Computed Tomographic Image Screening for Cystic Lung Diseases in Patients with Spontaneous Pneumothorax Is Cost Effective
- PMID: 27737563
- PMCID: PMC5461992
- DOI: 10.1513/AnnalsATS.201606-459OC
Chest Computed Tomographic Image Screening for Cystic Lung Diseases in Patients with Spontaneous Pneumothorax Is Cost Effective
Abstract
Rationale: Patients without a known history of lung disease presenting with a spontaneous pneumothorax are generally diagnosed as having primary spontaneous pneumothorax. However, occult diffuse cystic lung diseases such as Birt-Hogg-Dubé syndrome (BHD), lymphangioleiomyomatosis (LAM), and pulmonary Langerhans cell histiocytosis (PLCH) can also first present with a spontaneous pneumothorax, and their early identification by high-resolution computed tomographic (HRCT) chest imaging has implications for subsequent management.
Objectives: The objective of our study was to evaluate the cost-effectiveness of HRCT chest imaging to facilitate early diagnosis of LAM, BHD, and PLCH.
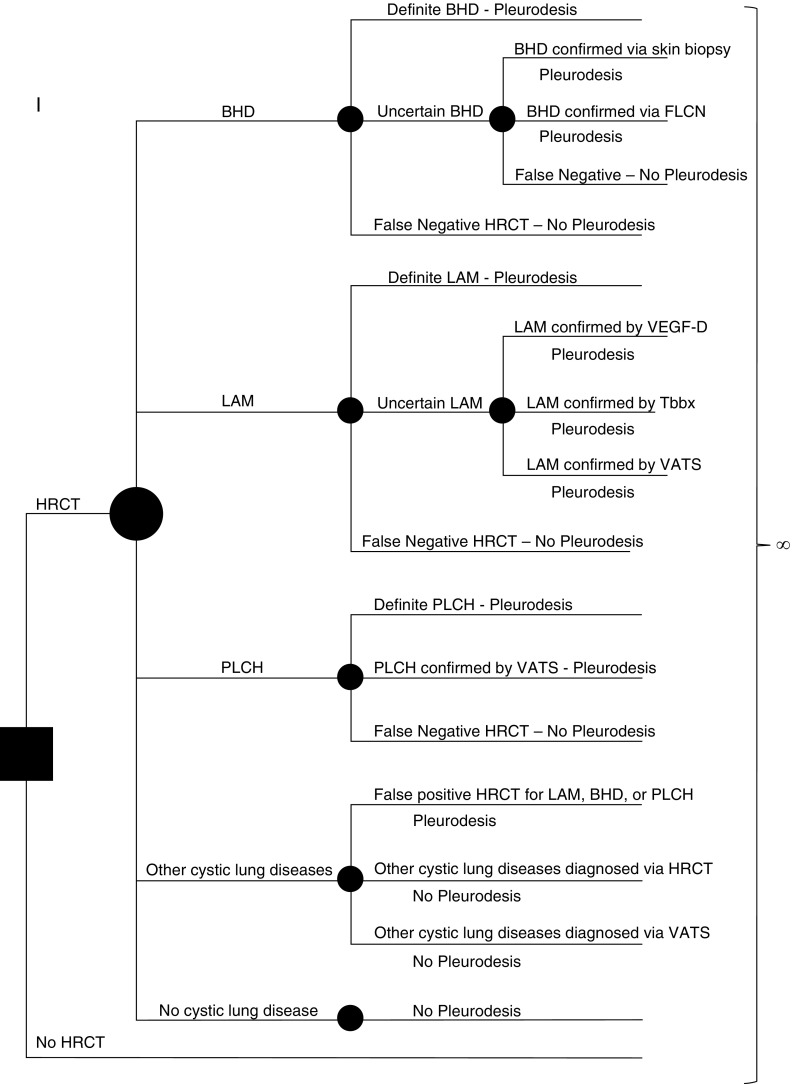
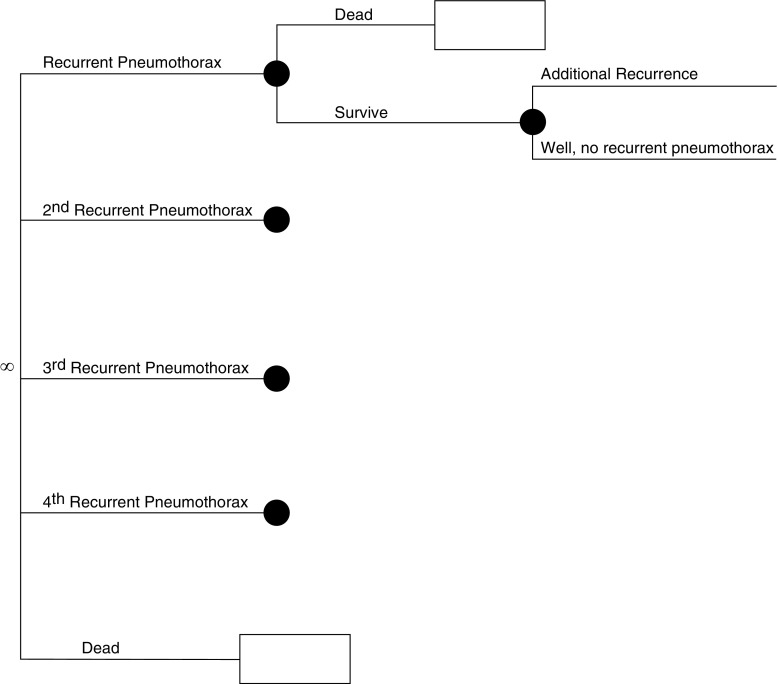
Methods: We constructed a Markov state-transition model to assess the cost-effectiveness of screening HRCT to facilitate early diagnosis of diffuse cystic lung diseases in patients presenting with an apparent primary spontaneous pneumothorax. Baseline data for prevalence of BHD, LAM, and PLCH and rates of recurrent pneumothoraces in each of these diseases were derived from the literature. Costs were extracted from 2014 Medicare data. We compared a strategy of HRCT screening followed by pleurodesis in patients with LAM, BHD, or PLCH versus conventional management with no HRCT screening.
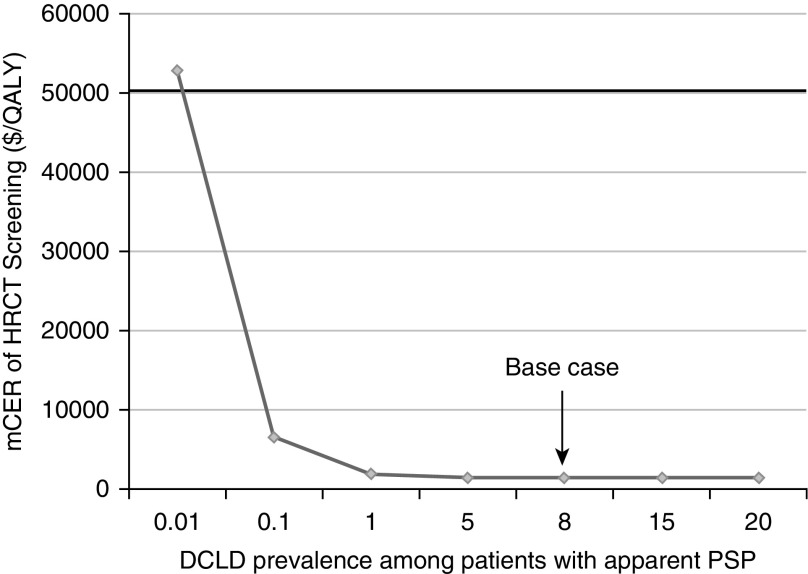
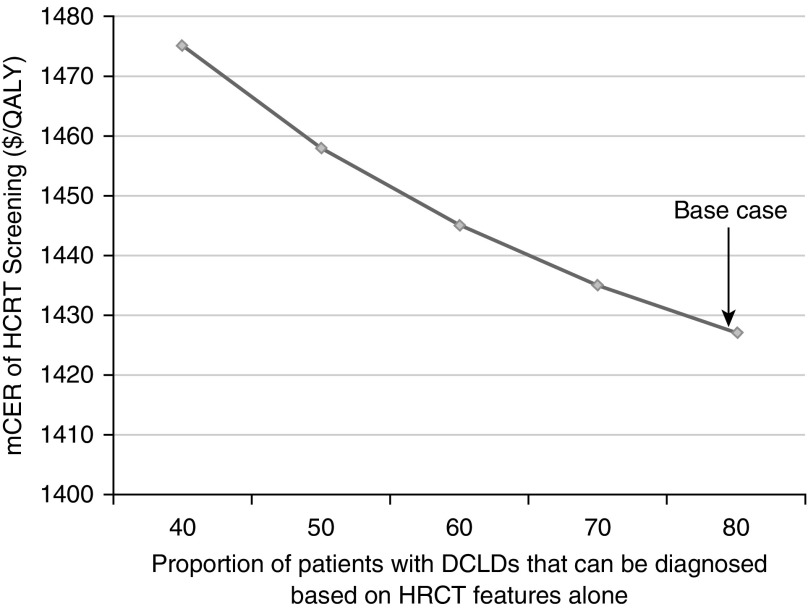
Measurements and main results: In our base case analysis, screening for the presence of BHD, LAM, or PLCH in patients presenting with a spontaneous pneumothorax was cost effective, with a marginal cost-effectiveness ratio of $1,427 per quality-adjusted life-year gained. Sensitivity analysis showed that screening HRCT remained cost effective for diffuse cystic lung diseases prevalence as low as 0.01%.
Conclusions: HRCT image screening for BHD, LAM, and PLCH in patients with apparent primary spontaneous pneumothorax is cost effective. Clinicians should consider performing a screening HRCT in patients presenting with apparent primary spontaneous pneumothorax.
Keywords: Birt-Hogg-Dubé syndrome; lymphangioleiomyomatosis; pneumothorax; pulmonary Langerhans cell histiocytosis.
Figures
Comment in
-
First Spontaneous Pneumothorax: Time for Screening High-Resolution Computed Tomographic Imaging to Look for Cystic Lung Disease?Ann Am Thorac Soc. 2017 Jan;14(1):12-13. doi: 10.1513/AnnalsATS.201610-814ED. Ann Am Thorac Soc. 2017. PMID: 28035875 No abstract available.
References
-
- Melton LJ, III, Hepper NG, Offord KP. Incidence of spontaneous pneumothorax in Olmsted County, Minnesota: 1950 to 1974. Am Rev Respir Dis. 1979;120:1379–1382. - PubMed
-
- Baumann MH, Strange C, Heffner JE, Light R, Kirby TJ, Klein J, Luketich JD, Panacek EA, Sahn SA, Group APC AACP Pneumothorax Consensus Group. Management of spontaneous pneumothorax: an American College of Chest Physicians Delphi consensus statement. Chest. 2001;119:590–602. - PubMed
-
- Bintcliffe OJ, Hallifax RJ, Edey A, Feller-Kopman D, Lee YC, Marquette CH, Tschopp JM, West D, Rahman NM, Maskell NA. Spontaneous pneumothorax: time to rethink management? Lancet Respir Med. 2015;3:578–588. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
