

Management of delayed cerebral ischemia after subarachnoid hemorrhage
- PMID: 27737684
- PMCID: PMC5064957
- DOI: 10.1186/s13054-016-1447-6
Management of delayed cerebral ischemia after subarachnoid hemorrhage
Abstract
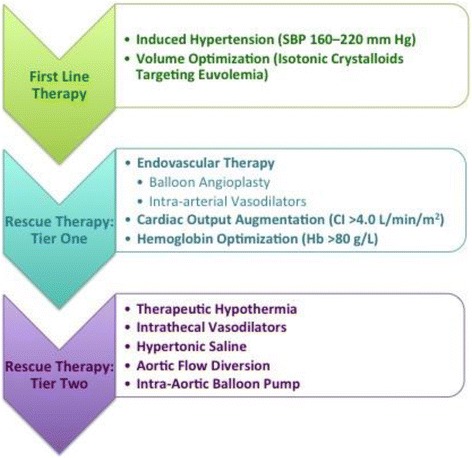
For patients who survive the initial bleeding event of a ruptured brain aneurysm, delayed cerebral ischemia (DCI) is one of the most important causes of mortality and poor neurological outcome. New insights in the last decade have led to an important paradigm shift in the understanding of DCI pathogenesis. Large-vessel cerebral vasospasm has been challenged as the sole causal mechanism; new hypotheses now focus on the early brain injury, microcirculatory dysfunction, impaired autoregulation, and spreading depolarization. Prevention of DCI primarily relies on nimodipine administration and optimization of blood volume and cardiac performance. Neurological monitoring is essential for early DCI detection and intervention. Serial clinical examination combined with intermittent transcranial Doppler ultrasonography and CT angiography (with or without perfusion) is the most commonly used monitoring paradigm, and usually suffices in good grade patients. By contrast, poor grade patients (WFNS grades 4 and 5) require more advanced monitoring because stupor and coma reduce sensitivity to the effects of ischemia. Greater reliance on CT perfusion imaging, continuous electroencephalography, and invasive brain multimodality monitoring are potential strategies to improve situational awareness as it relates to detecting DCI. Pharmacologically-induced hypertension combined with volume is the established first-line therapy for DCI; a good clinical response with reversal of the presenting deficit occurs in 70 % of patients. Medically refractory DCI, defined as failure to respond adequately to these measures, should trigger step-wise escalation of rescue therapy. Level 1 rescue therapy consists of cardiac output optimization, hemoglobin optimization, and endovascular intervention, including angioplasty and intra-arterial vasodilator infusion. In highly refractory cases, level 2 rescue therapies are also considered, none of which have been validated. This review provides an overview of current state-of-the-art care for DCI management.
Keywords: Delayed cerebral ischemia; Multimodality monitoring; Subarachnoid hemorrhage; Vasospasm.
Figures

References
-
- Etminan N, DI Vergouwen M, Ilodigwe D, Macdonald RL. Effect of pharmaceutical treatment on vasospasm, delayed cerebral ischemia, and clinical outcome in patients with aneurysmal subarachnoid hemorrhage: a systematic review and meta-analysis. J Cereb Blood Flow Metab. 2011;31(6):1443–51. doi: 10.1038/jcbfm.2011.7. - DOI - PMC - PubMed
-
- Macdonald RL, Higashida RT, Keller E, Mayer SA, Molyneux A, Raabe A, Vajkoczy P, Wanke I, Bach D, Frey A, Marr A, Roux S, Kassell N. Clazosentan, an endothelin receptor antagonist, in patients with aneurysmal subarachnoid haemorrhage undergoing surgical clipping: a randomised, double-blind, placebo-controlled phase 3 trial (CONSCIOUS-2) Lancet Neurol. 2011;10(7):618–25. doi: 10.1016/S1474-4422(11)70108-9. - DOI - PubMed
-
- Petruck KC, West M, Mohr G, Weir BK, Benoit BG, Gentilli F, Disney LB, Khan MI, Grace M, Holness RO, Karwon MS, Ford RM, Cameron S, Tucker WS, Purves GB, Miller JDR, Hunter KM, Richard MT, Durity FA, Chan R, Cleain LJ, Maroun FB, Godon A. Nimodipine treatment in poor-grade aneurysm patients. J Neurosurg. 1988;68:505–17. doi: 10.3171/jns.1988.68.4.0505. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
