

Reconciliation of Type 2 Diabetes Remission Rates in Studies of Roux-en-Y Gastric Bypass
- PMID: 27737910
- PMCID: PMC5127233
- DOI: 10.2337/dc16-0954
Reconciliation of Type 2 Diabetes Remission Rates in Studies of Roux-en-Y Gastric Bypass
Abstract
Objective: Bariatric surgery may induce remission of type 2 diabetes in obese patients. However, estimates of remission rates reported in the literature range from 25 to 81%, contributing to the uncertainty patients and physicians both face as they assess treatment options. This analysis attempts to reconcile the seemingly disparate rates of diabetes remission reported in studies of Roux-en-Y gastric bypass (RYGB) surgery. It examines variation in the methodologies used to derive the estimates and proposes outcomes that should be reported by all studies.
Research design and methods: A literature review yielded 10 large (n > 100), recent (index surgery since 2000) studies of diabetes remission after RYGB. These studies differed in definitions of remission (partial vs. complete), lengths of follow-up (1 year vs. ≥3 years), reported outcomes (cumulative vs. prevalent remission), and risks of attrition bias.
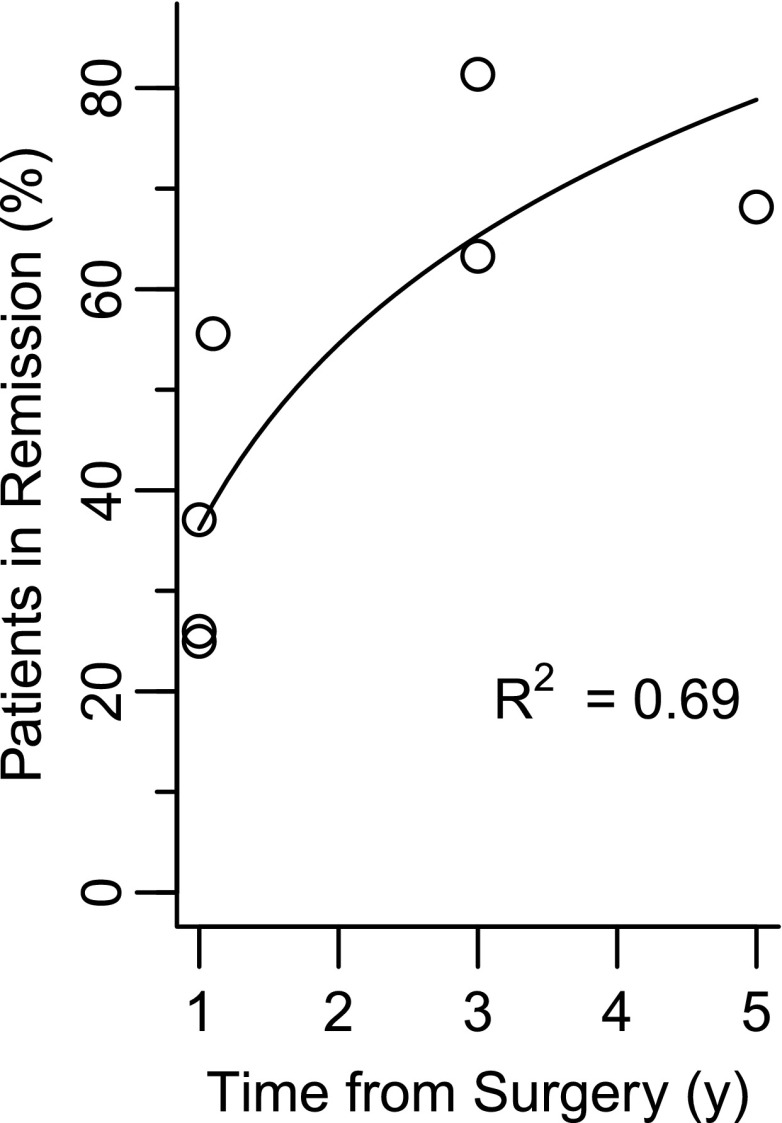
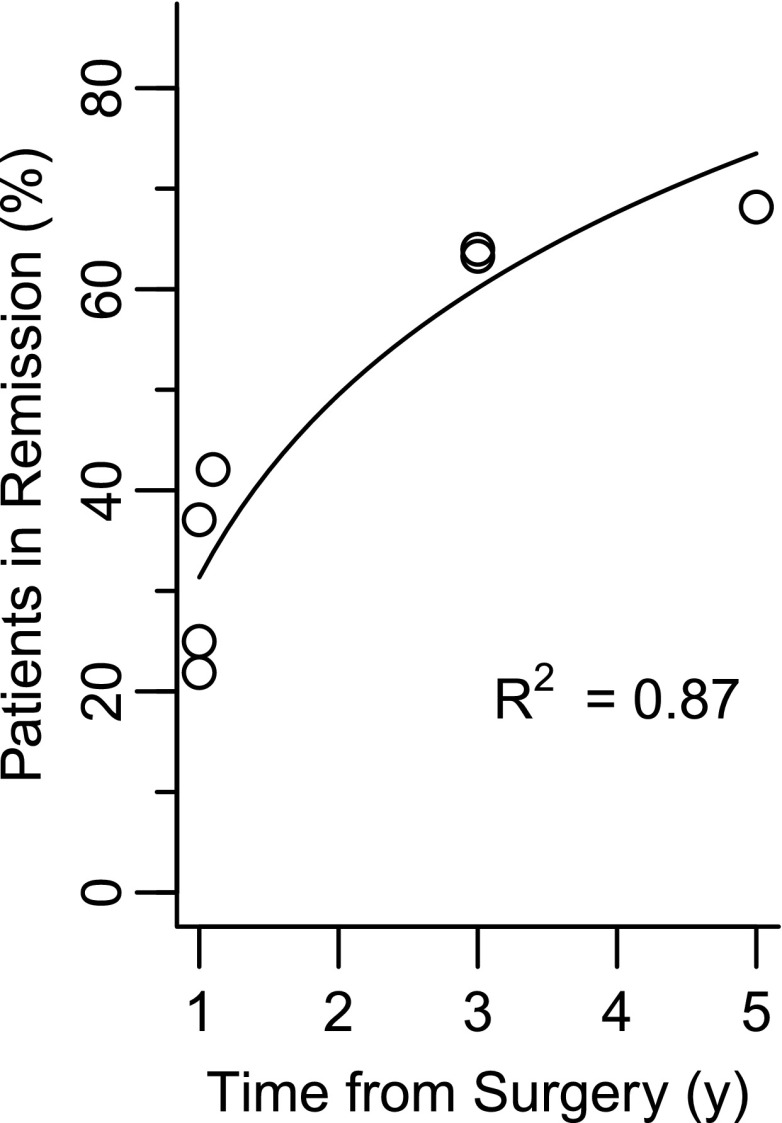
Results: Reported rates of partial remission were 10-30 percentage points higher than rates of complete remission. Study duration explained 69% of the variability in cumulative remission rates, plateauing at 3 years. Adjustment for attrition increased the explained variability to 87%. Attrition-adjusted, 3-year cumulative, complete remission rates ranged from 63 to 65%; however, this does not account for relapse. Attrition-adjusted, 3-year prevalent complete remission rates that accounted for relapse were 23%.
Conclusions: Variations in reported rates of diabetes remission after RYGB are primarily related to definitions and study duration. Future studies should report both cumulative and prevalent remission to aid decision making and more easily compare studies.
© 2016 by the American Diabetes Association.
Figures
References
-
- Rubino F, Nathan DM, Eckel RH, et al. .; Delegates of the 2nd Diabetes Surgery Summit . Metabolic surgery in the treatment algorithm for type 2 diabetes: a joint statement by international diabetes organizations. Diabetes Care 2016;39:861–877 - PubMed
-
- Buchwald H, Estok R, Fahrbach K, et al. Weight and type 2 diabetes after bariatric surgery: systematic review and meta-analysis. Am J Med 2009;122:248–256.e5 - PubMed
-
- Yu J, Zhou X, Li L, et al. The long-term effects of bariatric surgery for type 2 diabetes: systematic review and meta-analysis of randomized and non-randomized evidence. Obes Surg 2015;25:143–158 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
