

Hyperammonemia: What Urea-lly Need to Know: Case Report of Severe Noncirrhotic Hyperammonemic Encephalopathy and Review of the Literature
- PMID: 27738433
- PMCID: PMC5050374
- DOI: 10.1155/2016/8512721
Hyperammonemia: What Urea-lly Need to Know: Case Report of Severe Noncirrhotic Hyperammonemic Encephalopathy and Review of the Literature
Abstract
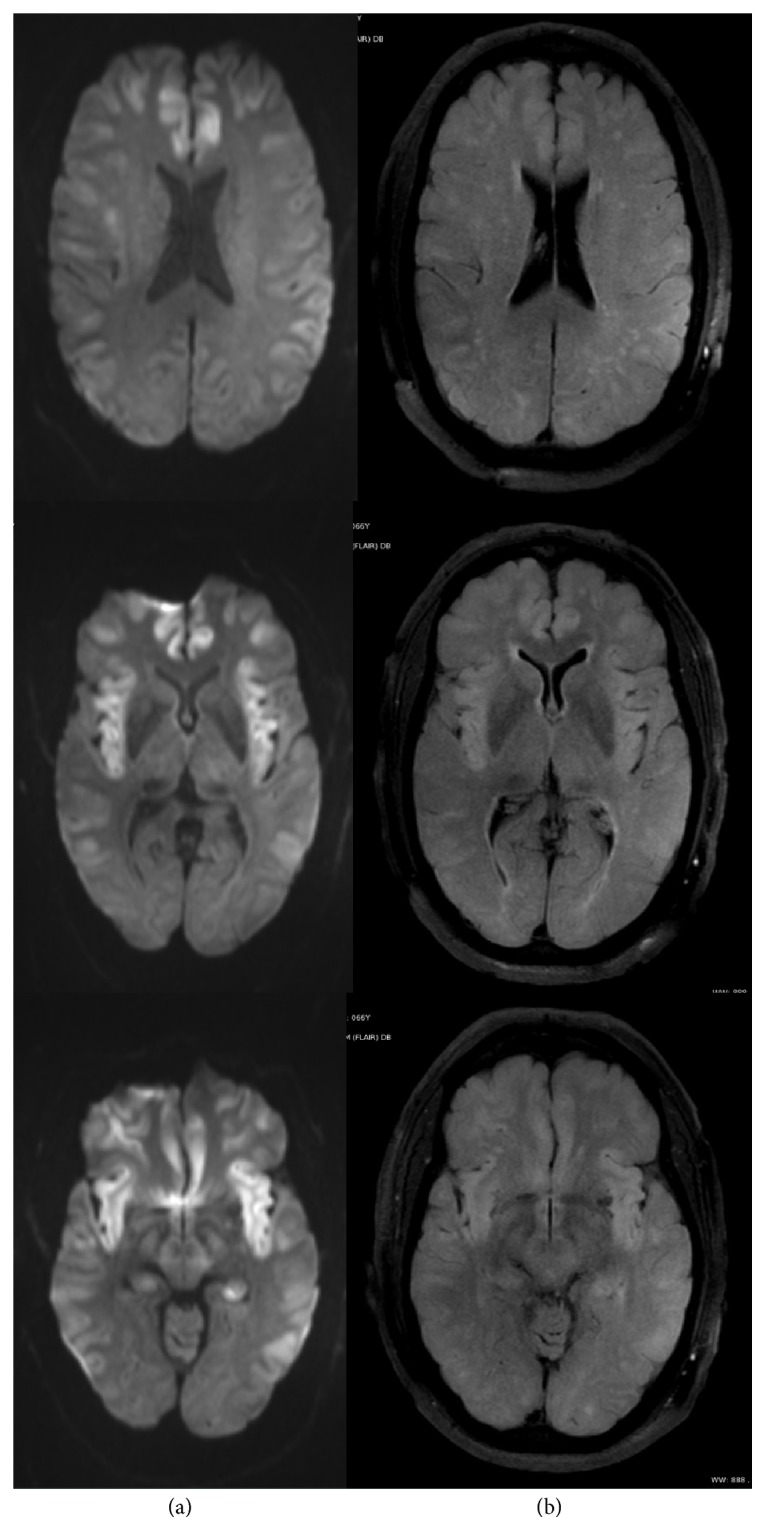
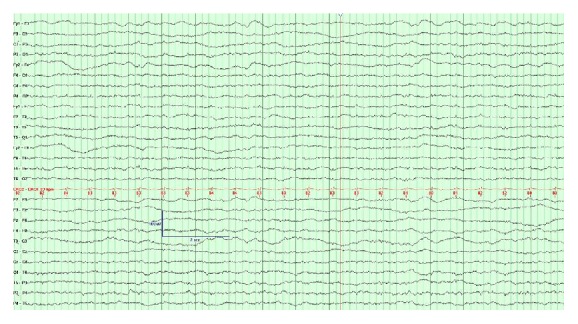
Purpose. A 66-year-old man who presented with coma was found to have isolated severe hyperammonemia and diagnosed with a late-onset urea-cycle disorder. He was treated successfully and had full recovery. Methods. We report a novel case of noncirrhotic hyperammonemia and review the literature on this topic. Selected literature for review included English-language articles concerning hyperammonemia using the search terms "hyperammonemic encephalopathy", "non-cirrhotic encephalopathy", "hepatic encephalopathy", "urea-cycle disorders", "ornithine transcarbamylase (OTC) deficiency", and "fulminant hepatic failure". Results. A unique case of isolated hyperammonemia diagnosed as late-onset OTC deficiency is presented. Existing evidence about hyperammonemia is organized to address pathophysiology, clinical presentation, diagnosis, and treatment. The case report is discussed in context of the reviewed literature. Conclusion. Late-onset OTC deficiency presenting with severe hyperammonemic encephalopathy and extensive imaging correlate can be fully reversible if recognized promptly and treated aggressively.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
