

Home-based versus centre-based cardiac rehabilitation: abridged Cochrane systematic review and meta-analysis
- PMID: 27738516
- PMCID: PMC5030549
- DOI: 10.1136/openhrt-2016-000463
Home-based versus centre-based cardiac rehabilitation: abridged Cochrane systematic review and meta-analysis
Abstract
Objective: To update the Cochrane review comparing the effects of home-based and supervised centre-based cardiac rehabilitation (CR) on mortality and morbidity, quality of life, and modifiable cardiac risk factors in patients with heart disease.
Methods: Systematic review and meta-analysis. The Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, EMBASE, PsycINFO and CINAHL were searched up to October 2014, without language restriction. Randomised trials comparing home-based and centre-based CR programmes in adults with myocardial infarction, angina, heart failure or who had undergone coronary revascularisation were included.
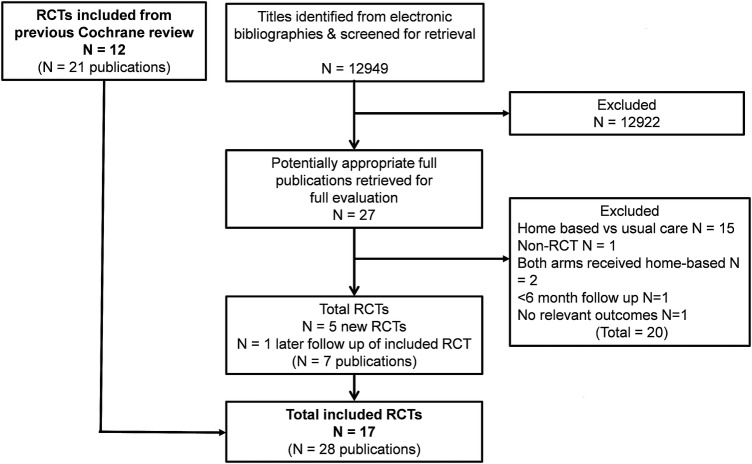
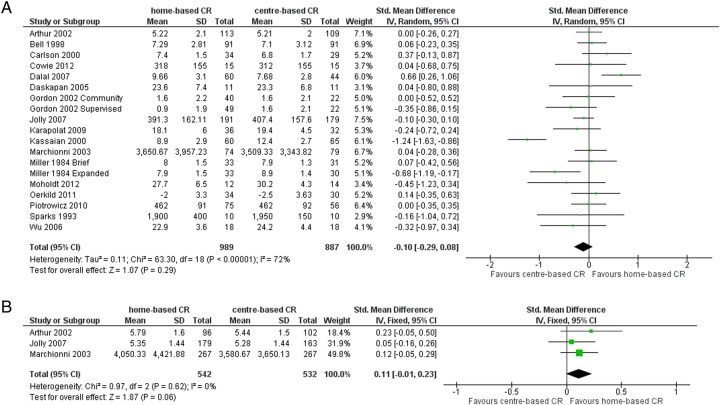
Results: 17 studies with 2172 patients were included. No difference was seen between home-based and centre-based CR in terms of: mortality (relative risk (RR) 0.79, 95% CI 0.43 to 1.47); cardiac events; exercise capacity (mean difference (MD) -0.10, -0.29 to 0.08); total cholesterol (MD 0.07 mmol/L, -0.24 to 0.11); low-density lipoprotein cholesterol (MD -0.06 mmol/L, -0.27 to 0.15); triglycerides (MD -0.16 mmol/L, -0.38 to 0.07); systolic blood pressure (MD 0.2 mm Hg, -3.4 to 3.8); smoking (RR 0.98, 0.79 to 1.21); health-related quality of life and healthcare costs. Lower high-density lipoprotein cholesterol (MD -0.07 mmol/L, -0.11 to -0.03, p=0.001) and lower diastolic blood pressure (MD -1.9 mm Hg, -0.8 to -3.0, p=0.009) were observed in centre-based participants. Home-based CR was associated with slightly higher adherence (RR 1.04, 95% CI 1.01 to 1.07).
Conclusions: Home-based and centre-based CR provide similar benefits in terms of clinical and health-related quality of life outcomes at equivalent cost for those with heart failure and following myocardial infarction and revascularisation.
Keywords: CORONARY ARTERY DISEASE; HEART FAILURE.
Figures
References
-
- World Health Organization (WHO) 2015. WHO Mortality Database: 25 November 2015. http://www.who.int/healthinfo/statistics/mortality_rawdata/en/index.html (accessed 25 May 2016).
-
- British Heart Foundation (BHF). Heart statistics 2015. http://www.bhf.org.uk/research/heart-statistics (accessed 22 Dec 2015).
-
- Balady GJ, Williams MA, Ades PA et al. , American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee; Council on Clinical Cardiology; Councils on Cardiovascular Nursing, Epidemiology and Prevention, and Nutrition, Physical Activity, and Metabolism; American Association of Cardiovascular and Pulmonary Rehabilitation. Core components of cardiac rehabilitation/secondary prevention programs: 2007 update: a scientific statement from the American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee, the Council on Clinical Cardiology; the councils on Cardiovascular Nursing, Epidemiology and Prevention, and Nutrition, Physical Activity, and Metabolism; and the American Association of Cardiovascular and Pulmonary Rehabilitation . J Cardiopulm Rehabil Prev 2007;27:121–9. - PubMed
-
- Piepoli M, Maugeri FS, Campana M et al. . Experience from controlled trials of physical training in chronic heart failure. Protocol and patient factors in effectiveness in the improvement of exercise tolerance. Eur Heart J 1998;19:466–75. - PubMed
-
- Piepoli MF, Corrà U, Benzer W et al. , Cardiac Rehabilitation Section of the European Association of Cardiovascular Prevention and Rehabilitation. Secondary prevention through cardiac rehabilitation: from knowledge to implementation. A position paper from the Cardiac Rehabilitation Section of the European Association of Cardiovascular Prevention and Rehabilitation. Eur J Cardiovasc Prev Rehabil 2010;17:1–17. 10.1097/HJR.0b013e3283313592 - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical