

Respiratory syncytial virus a and b display different temporal patterns in a 4-year prospective cross-sectional study among children with acute respiratory infection in a tropical city
- PMID: 27741144
- PMCID: PMC5072971
- DOI: 10.1097/MD.0000000000005142
Respiratory syncytial virus a and b display different temporal patterns in a 4-year prospective cross-sectional study among children with acute respiratory infection in a tropical city
Abstract
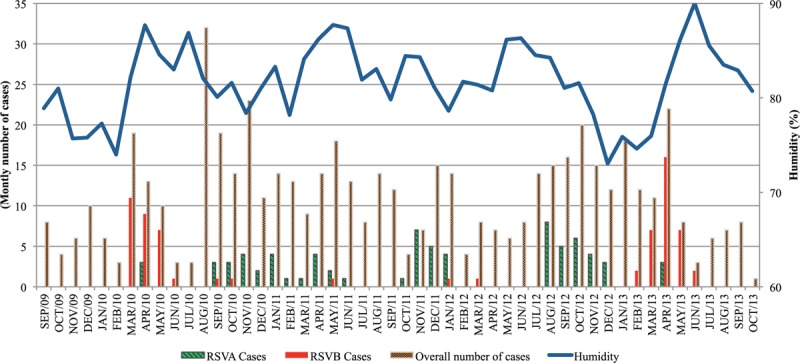
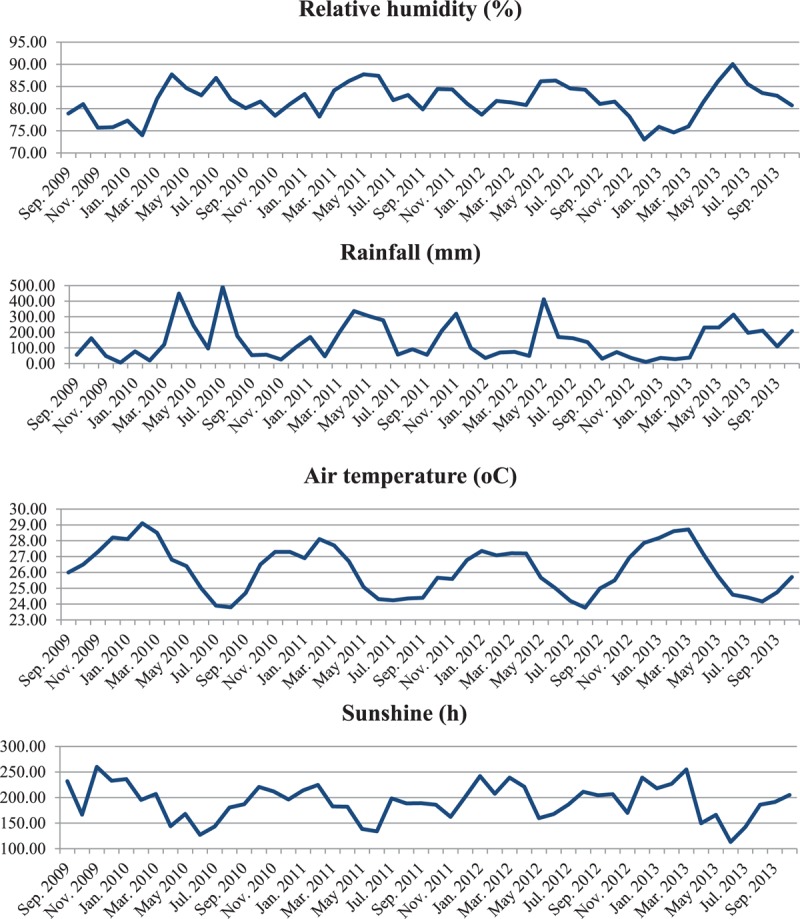
Respiratory syncytial virus (RSV) is one of the most common etiological agents of childhood respiratory infections globally. Information on seasonality of different antigenic groups is scarce. We aimed to describe the frequency, seasonality, and age of children infected by RSV antigenic groups A (RSVA) and B (RSVB) among children with ARI in a 4-year period.Children (6-23 months old) with respiratory infection for ≤7 days were enrolled in a prospective cross-sectional study, from September, 2009 to October, 2013, in Salvador, in a tropical region of Brazil. Upon recruitment, demographic, clinical data, and nasopharyngeal aspirates (NPA) were collected. A multiplex quantitative real-time polymerase chain reaction (RT-PCR) with a group-specific primer and probeset for RSVA and RSVB was used. Seasonal distribution of infection by RSV different antigenic groups was evaluated by Prais-Wisten regression.Of 560 cases, the mean age was 11.4 ± 4.5 months and there were 287 (51.3%) girls. Overall, RSV was detected in 139 (24.8%; 95% CI: 21.4%-28.5%) cases, RSVA in 74 (13.2%; 95% CI: 10.6%-16.2%) cases, and RSVB in 67 (12.0%; 95% CI: 9.5%-14.9%) cases. Two (0.4%; 95% CI: 0.06%-1.2%) cases had coinfection. RSVA frequency was 9.6%, 18.4%, 21.6%, and 3.1% in 2010, 2011, 2012, and 2013, respectively. RSVB frequency was 19.2%, 0.7%, 1.4%, and 35.4% in the same years. RSVA was more frequently found from August to January than February to July (18.2% vs. 6.4%, P < 0.001). RSVB was more frequently found (P < 0.001) between March and June (36.0%) than July to October (1.0%) or November to February (1.6%). RSVB infection showed seasonal distribution and positive association with humidity (P = 0.02) whereas RSVA did not. RSVA was more common among children ≥1-year-old (17.8% vs. 1.8%; P = 0.02), as opposed to RSVB (11.5% vs. 12.2%; P = 0.8).One quarter of patients had RSV infection. RSVA compromised more frequently children aged ≥1 year. RSVA predominated in 2011 and 2012 whereas RSVB predominated in 2010 and 2013. In regard to months, RSVA was more frequent from August to January whereas RSVB was more often detected between March and June. Markedly different monthly as well as yearly patterns for RSVA and RSVB reveal independent RSV antigenic groups' epidemics.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Nascimento-Carvalho CM, Cardoso MRA, Barral A, et al. Seasonal patterns of viral and bacterial infections among children hospitalized with community-acquired pneumonia in a tropical region. Scan J Infect Dis 2010; 42:839–844. - PubMed
-
- Kimberlin DW, Brady MT, Jackson MA, Long SS. American Academy of Pediatrics. Respiratory syncytial virus: initiation and termination of immunoprophylaxis. Red Bood: 2015 Report of the Committee on Infectious Diseases 30th ed.Elk Grove Village, IL: American Academy of Pediatrics; 2015. 672.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
