

Airway pressure release ventilation during ex vivo lung perfusion attenuates injury
- PMID: 27742245
- PMCID: PMC5164862
- DOI: 10.1016/j.jtcvs.2016.09.029
Airway pressure release ventilation during ex vivo lung perfusion attenuates injury
Abstract
Objective: Critical organ shortages have resulted in ex vivo lung perfusion gaining clinical acceptance for lung evaluation and rehabilitation to expand the use of donation after circulatory death organs for lung transplantation. We hypothesized that an innovative use of airway pressure release ventilation during ex vivo lung perfusion improves lung function after transplantation.
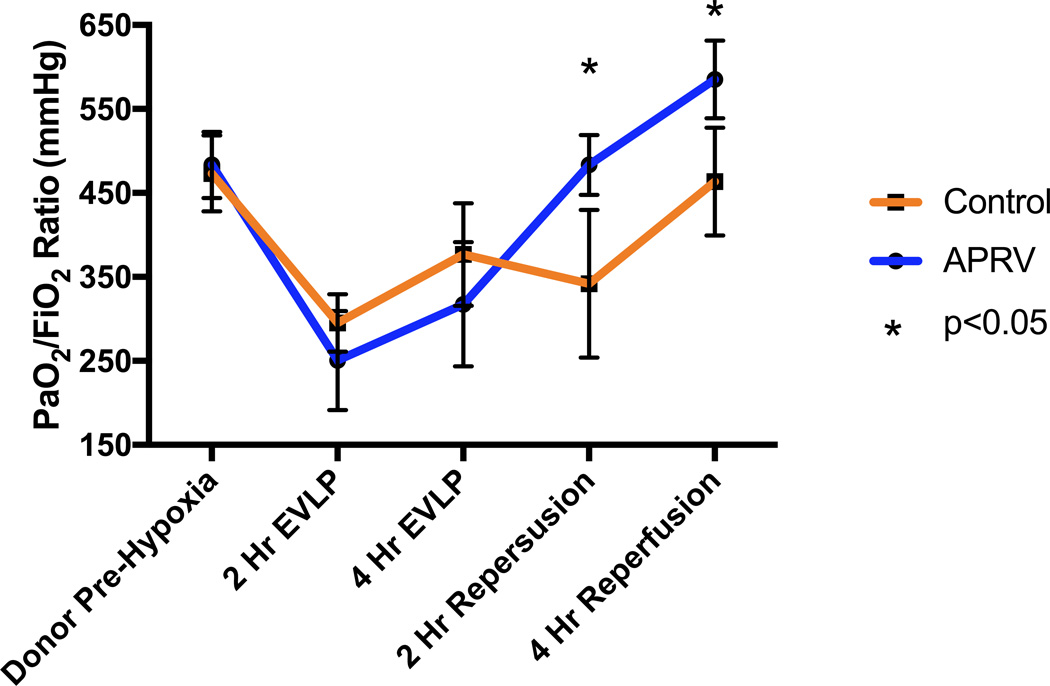
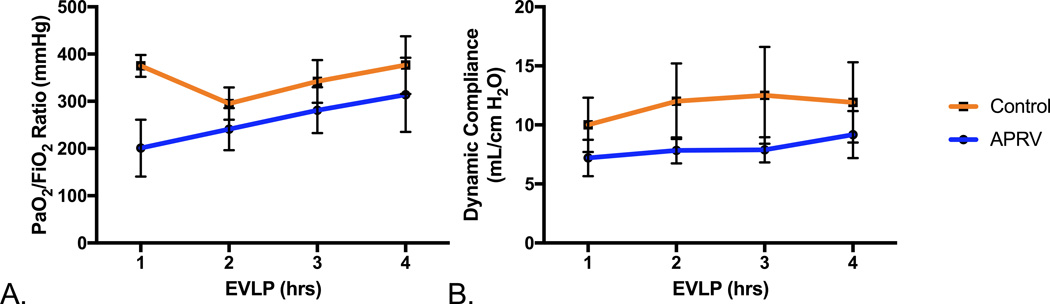
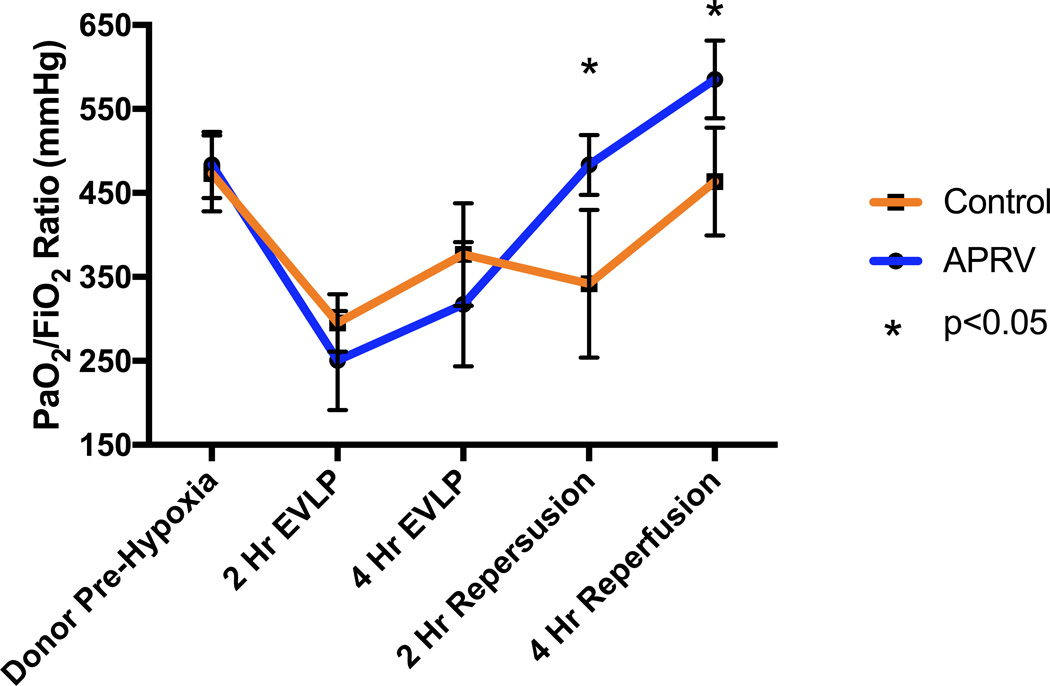
Methods: Two groups (n = 4 animals/group) of porcine donation after circulatory death donor lungs were procured after hypoxic cardiac arrest and a 2-hour period of warm ischemia, followed by a 4-hour period of ex vivo lung perfusion rehabilitation with standard conventional volume-based ventilation or pressure-based airway pressure release ventilation. Left lungs were subsequently transplanted into recipient animals and reperfused for 4 hours. Blood gases for partial pressure of oxygen/inspired oxygen fraction ratios, airway pressures for calculation of compliance, and percent wet weight gain during ex vivo lung perfusion and reperfusion were measured.
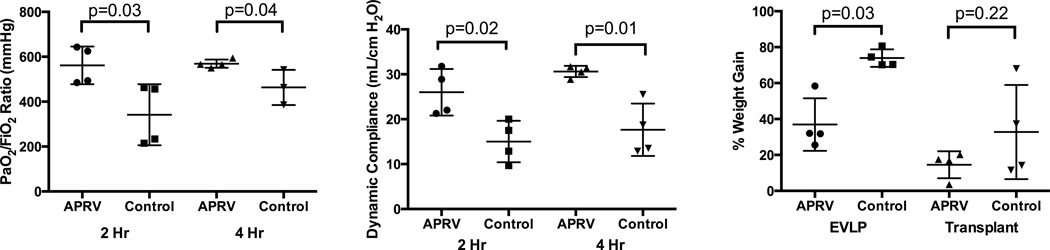
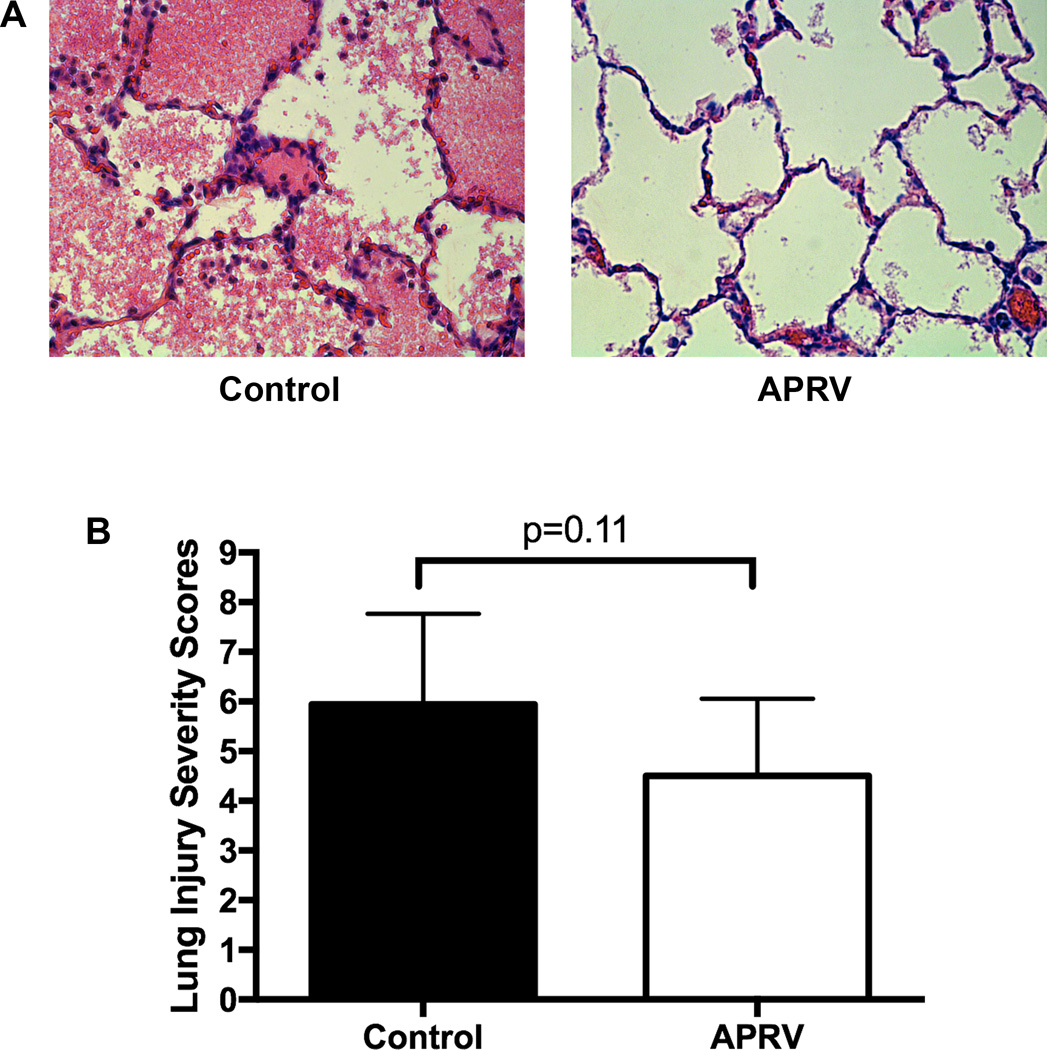
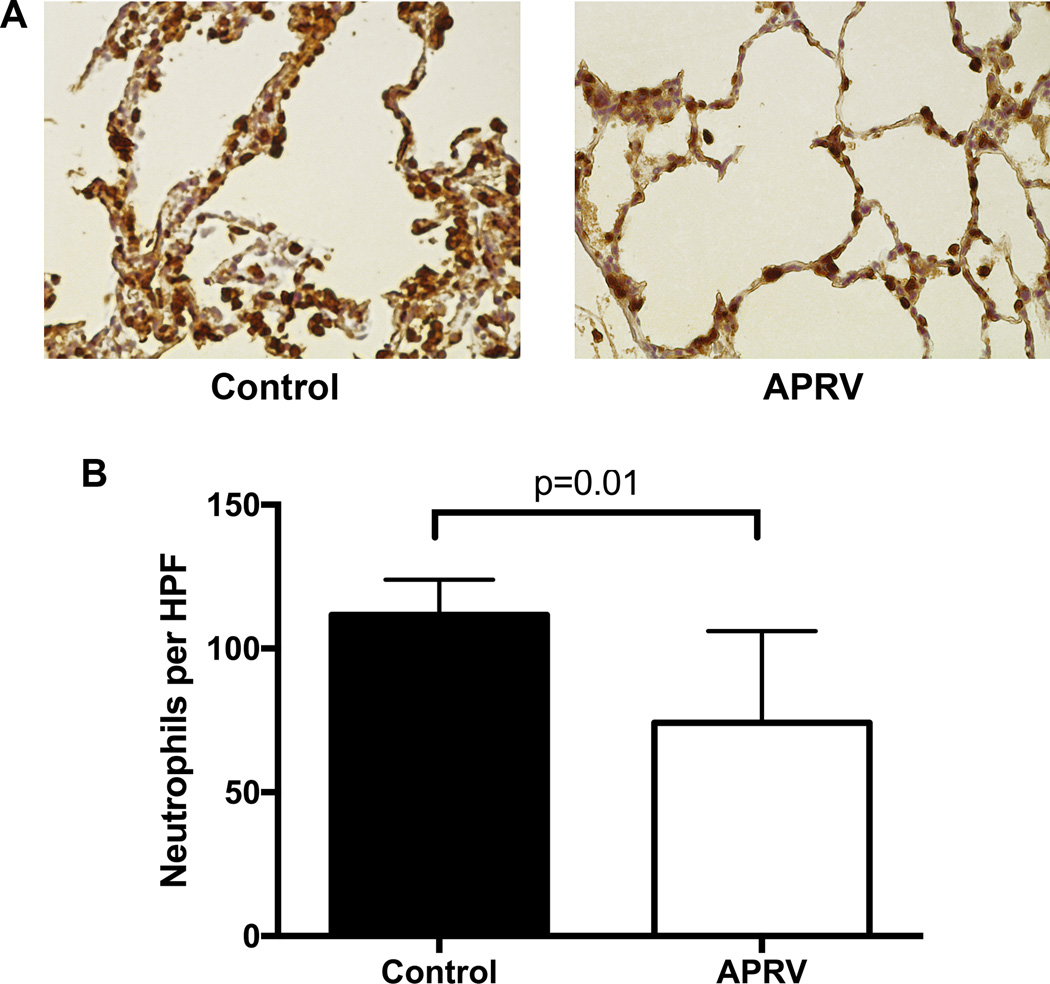
Results: Airway pressure release ventilation during ex vivo lung perfusion significantly improved left lung oxygenation at 2 hours (561.5 ± 83.9 mm Hg vs 341.1 ± 136.1 mm Hg) and 4 hours (569.1 ± 18.3 mm Hg vs 463.5 ± 78.4 mm Hg). Likewise, compliance was significantly higher at 2 hours (26.0 ± 5.2 mL/cm H2O vs 15.0 ± 4.6 mL/cm H2O) and 4 hours (30.6 ± 1.3 mL/cm H2O vs 17.7 ± 5.9 mL/cm H2O) after transplantation. Finally, airway pressure release ventilation significantly reduced lung edema development on ex vivo lung perfusion on the basis of percentage of weight gain (36.9% ± 14.6% vs 73.9% ± 4.9%). There was no difference in additional edema accumulation 4 hours after reperfusion.
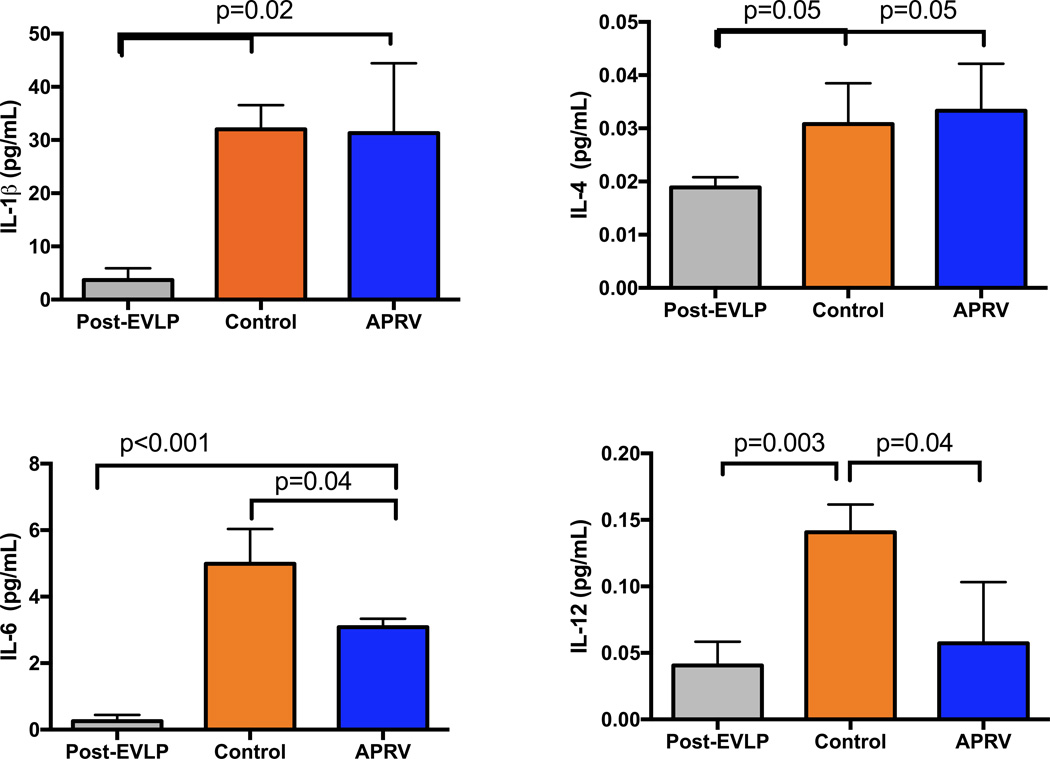
Conclusions: Pressure-directed airway pressure release ventilation strategy during ex vivo lung perfusion improves the rehabilitation of severely injured donation after circulatory death lungs. After transplant, these lungs demonstrate superior lung-specific oxygenation and dynamic compliance compared with lungs ventilated with standard conventional ventilation. This strategy, if implemented into clinical ex vivo lung perfusion protocols, could advance the field of donation after circulatory death lung rehabilitation to expand the lung donor pool.
Keywords: APRV; EVLP; airway pressure release ventilation; ex vivo lung perfusion; ischemia reperfusion; lung injury; lung transplant.
Copyright © 2016 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
There are no financial disclosures or conflicts of interest from any of the authors.
Figures
Comment in
-
Rescue, revive, rejuvenate: The new science of ex vivo lung perfusion.J Thorac Cardiovasc Surg. 2017 Jan;153(1):205. doi: 10.1016/j.jtcvs.2016.10.016. Epub 2016 Oct 22. J Thorac Cardiovasc Surg. 2017. PMID: 27838009 No abstract available.
References
-
- Christie JD, Edwards LB, Kucheryavaya AY, Aurora P, Dobbels F, Kirk R, et al. The Registry of the International Society for Heart and Lung Transplantation: twenty-seventh official adult lung and heart-lung transplant report--2010. J Heart Lung Transplant. 2010;29(10):1104–1118. - PubMed
-
- De Meester J, Smits JM, Persijn GG, Haverich A. Listing for lung transplantation: life expectancy and transplant effect, stratified by type of end-stage lung disease, the Eurotransplant experience. J Heart Lung Transplant. 2001;20(5):518–524. - PubMed
-
- Cypel M, Yeung JC, Hirayama S, Rubacha M, Fischer S, Anraku M, et al. Technique for prolonged normothermic ex vivo lung perfusion. J Heart Lung Transplant. 2008;27(12):1319–1325. - PubMed
-
- Steen S, Liao Q, Wierup PN, Bolys R, Pierre L, Sjoberg T. Transplantation of lungs from non-heart-beating donors after functional assessment ex vivo. Ann Thorac Surg. 2003;76(1):244–252. discussion 52. - PubMed
-
- Yeung JC, Cypel M, Waddell TK, van Raemdonck D, Keshavjee S. Update on donor assessment, resuscitation, and acceptance criteria, including novel techniques--non-heart-beating donor lung retrieval and ex vivo donor lung perfusion. Thorac Surg Clin. 2009;19(2):261–274. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
