

Simulated Online Adaptive Magnetic Resonance-Guided Stereotactic Body Radiation Therapy for the Treatment of Oligometastatic Disease of the Abdomen and Central Thorax: Characterization of Potential Advantages
- PMID: 27742541
- PMCID: PMC5376349
- DOI: 10.1016/j.ijrobp.2016.08.036
Simulated Online Adaptive Magnetic Resonance-Guided Stereotactic Body Radiation Therapy for the Treatment of Oligometastatic Disease of the Abdomen and Central Thorax: Characterization of Potential Advantages
Abstract
Purpose: To characterize potential advantages of online-adaptive magnetic resonance (MR)-guided stereotactic body radiation therapy (SBRT) to treat oligometastatic disease of the non-liver abdomen and central thorax.
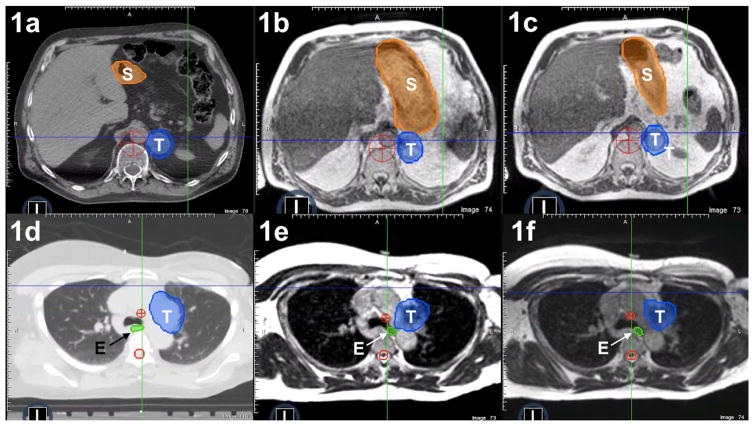
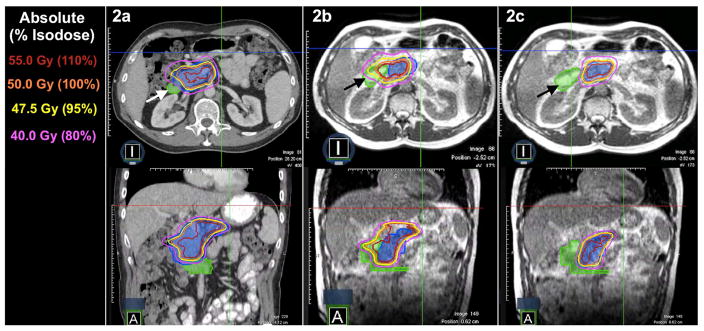
Methods and materials: Ten patients treated with RT for unresectable primary or oligometastatic disease of the non-liver abdomen (n=5) or central thorax (n=5) underwent imaging throughout treatment on a clinical MR image guided RT system. The SBRT plans were created on the basis of tumor/organ at risk (OAR) anatomy at initial computed tomography simulation (PI), and simulated adaptive plans were created on the basis of observed MR image set tumor/OAR "anatomy of the day" (PA). Each PA was planned under workflow constraints to simulate online-adaptive RT. Prescribed dose was 50 Gy/5 fractions, with goal coverage of 95% planning target volume (PTV) by 95% of the prescription, subject to hard OAR constraints. The PI was applied to each MR dataset and compared with PA to evaluate changes in dose delivered to tumor/OARs, with dose escalation when possible.
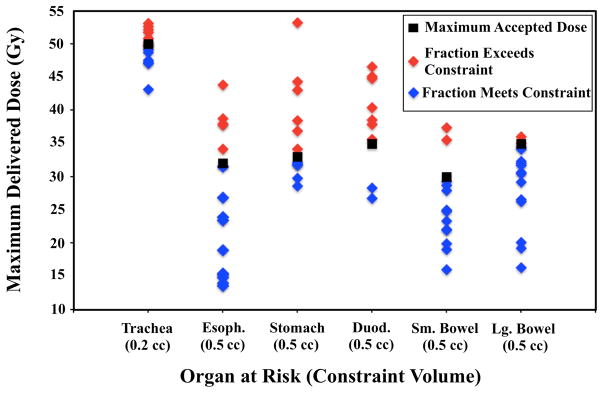
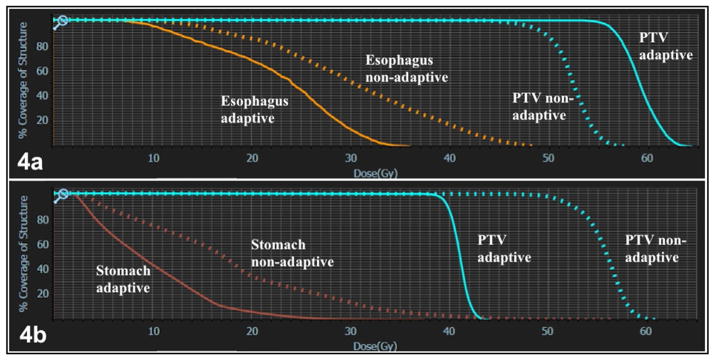
Results: Hard OAR constraints were met for all PIs based on anatomy from initial computed tomography simulation, and all PAs based on anatomy from each daily MR image set. Application of the PI to anatomy of the day caused OAR constraint violation in 19 of 30 cases. Adaptive planning increased PTV coverage in 21 of 30 cases, including 14 cases in which hard OAR constraints were violated by the nonadaptive plan. For 9 PA cases, decreased PTV coverage was required to meet hard OAR constraints that would have been violated in a nonadaptive setting.
Conclusions: Online-adaptive MRI-guided SBRT may allow PTV dose escalation and/or simultaneous OAR sparing compared with nonadaptive SBRT. A prospective clinical trial is underway at our institution to evaluate clinical outcomes of this technique.
Copyright © 2016 Elsevier Inc. All rights reserved.
Conflict of interest statement
Dr. Bradley reports departmental funding for clinical trials from ViewRay, and honoraria paid to Washington University by ViewRay for lectures he has given, outside of the submitted work.
Dr. Green reports honoraria from ViewRay, inc, outside the submitted work.
Dr. Henke reports grants from ViewRay Inc, outside the submitted work.
Dr. Jeffrey Olsen reports grants, personal fees and other from ViewRay, Inc, outside the submitted work.
Dr. Lindsey Olsen reports grants from Varian Medical Systems, outside the submitted work.
Dr. Kashani reports grants and personal fees from ViewRay Inc, outside the submitted work.
Dr. Mutic reports grants and other from ViewRay, Inc, grants and other from Varian Medical Systems, other from Philips Healthcare, other from Siemens, other from TreatSafely, LLC, and other from Radialogica, LLC, outside the submitted work.
Dr. Parikh reports grants from Philips Healthcare, grants and other from Varian Medical Systems, other from Holaira, Inc, other from Medtronic/Covidien, outside the submitted work.
Dr. Robinson reports grants and personal fees from Varian, grants from Elekta, personal fees from Radialogica, and personal fees from ViewRay, outside the submitted work;.
Dr. Wooten reports personal fees from ViewRay, Inc, outside the submitted work.
Dr. Yang reports grants from ViewRay and one software license agreement with ViewRay Inc, outside the submitted work.
Figures
References
-
- Potters L, Kavanagh B, Galvin JM, et al. American Society for Therapeutic Radiology and Oncology (ASTRO) and American College of Radiology (ACR) practice guideline for the performance of stereotactic body radiation therapy. Int J Radiat Oncol Biol Phys. 2010;76:326–332. - PubMed
-
- Timmerman RD, Kavanagh BD. Stereotactic body radiation therapy. Curr Probl Cancer. 2005;29:120–157. - PubMed
-
- Timmerman RD, Kavanagh BD, Cho LC, et al. Stereotactic body radiation therapy in multiple organ sites. J Clin Oncol. 2007;25:947–952. - PubMed
-
- Milano MT, Katz AW, Muhs AG, et al. A prospective pilot study of curative-intent stereotactic body radiation therapy in patients with 5 or fewer oligometastatic lesions. Cancer. 2008;112:650–658. - PubMed
-
- Salama JK, Hasselle MD, Chmura SJ, et al. Stereotactic body radiotherapy for multisite extracranial oligometastases: final report of a dose escalation trial in patients with 1 to 5 sites of metastatic disease. Cancer. 2012;118:2962–2970. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
