

Effect of Lung Transplantation on Health-Related Quality of Life in the Era of the Lung Allocation Score: A U.S. Prospective Cohort Study
- PMID: 27743488
- PMCID: PMC6085872
- DOI: 10.1111/ajt.14081
Effect of Lung Transplantation on Health-Related Quality of Life in the Era of the Lung Allocation Score: A U.S. Prospective Cohort Study
Abstract
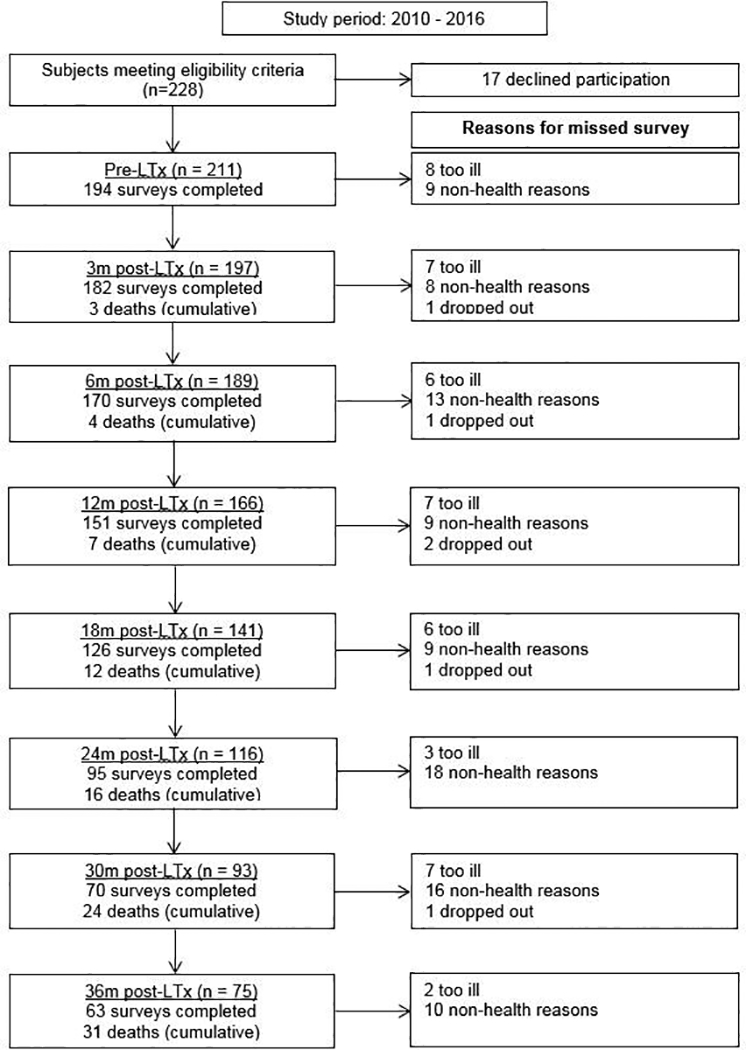
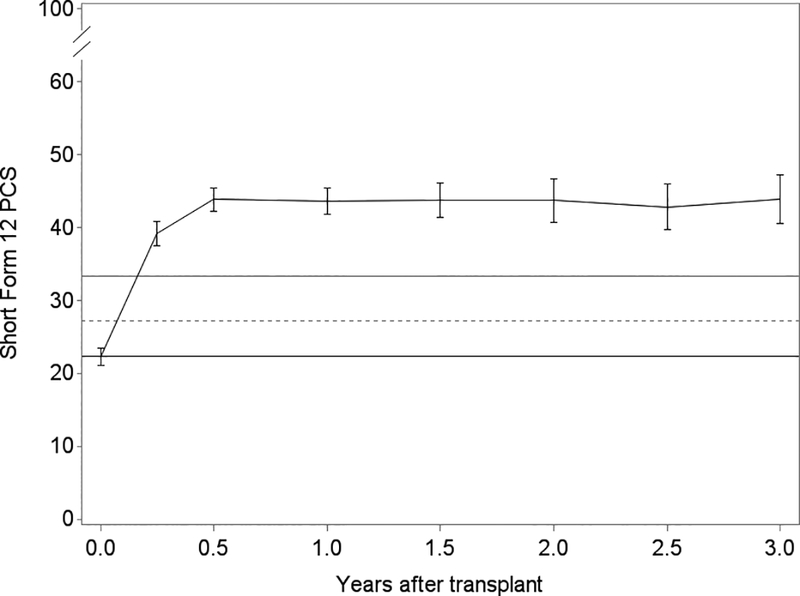
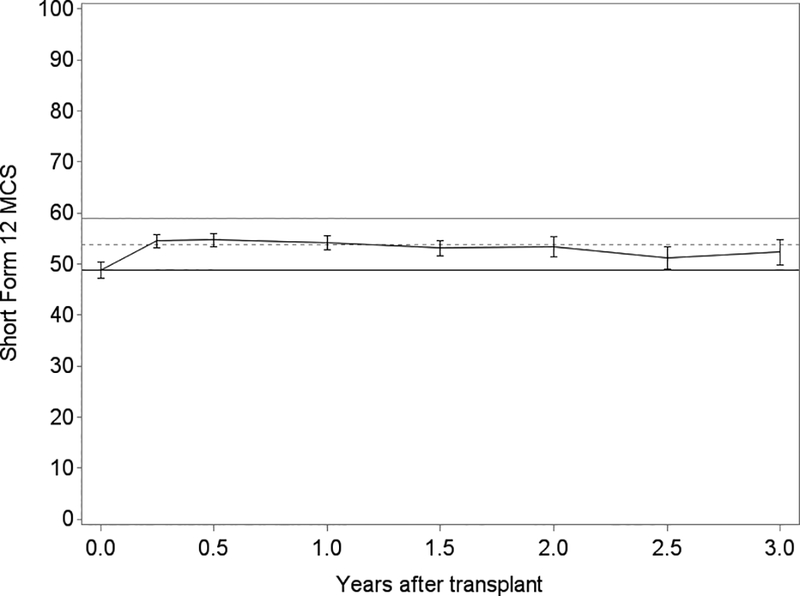
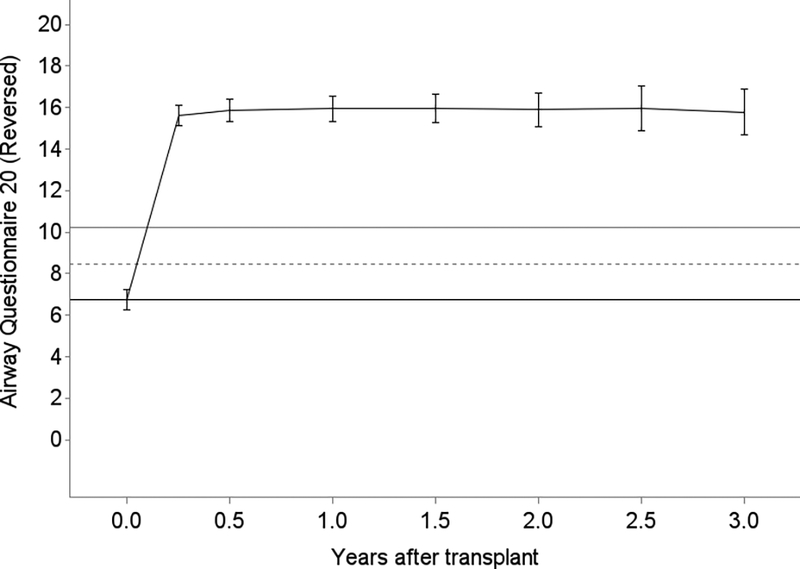
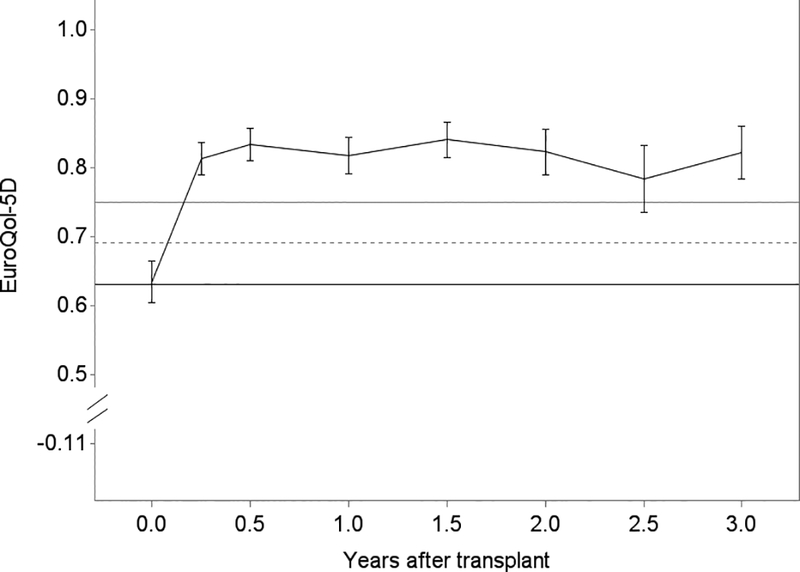
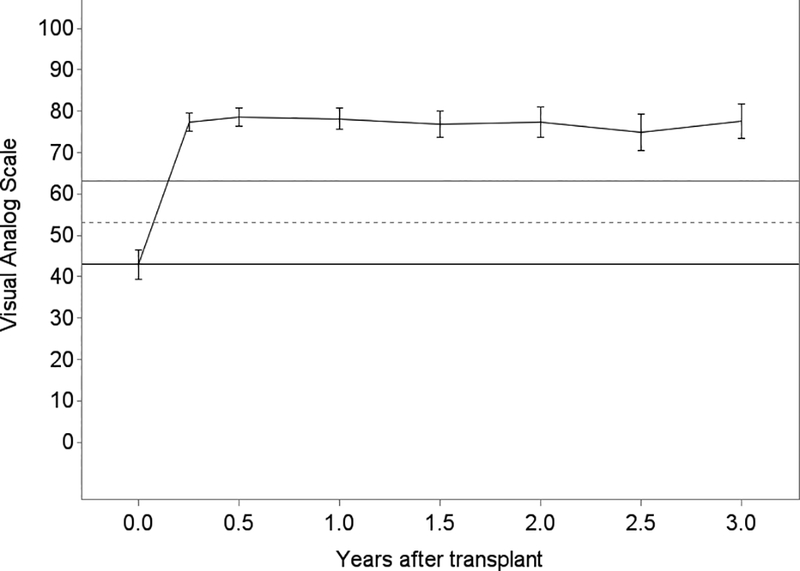
Under the U.S. Lung Allocation Score (LAS) system, older and sicker patients are prioritized for lung transplantation (LT). The impact of these changes on health-related quality of life (HRQL) after transplant has not been determined. In a single-center prospective cohort study from 2010 to 2016, we assessed HRQL before and repeatedly after LT for up to 3 years using the SF12-Physical and Mental Health, the respiratory-specific Airway Questionnaire 20-Revised, and the Euroqol 5D/Visual Analog Scale utility measures by multivariate linear mixed models jointly modeled with death. We also tested changes in LT-Valued Life Activities disability, BMI, allograft function, and 6-min walk test exercise capacity as predictors of HRQL change. Among 211 initial participants (92% of those eligible), LT improved HRQL by all 5 measures (p < 0.05) and all but SF12-Mental Health improved by threefold or greater than the minimally clinically important difference. Compared to younger participants, those aged ≥65 improved less in SF12-Physical and Mental Health (p < 0.01). Improvements in disability accounted for much of the HRQL improvement. In the LAS era, LT affords meaningful and durable HRQL improvements, mediated by amelioration of disability. Identifying factors limiting HRQL improvement in selected subgroups, especially those aged ≥65, are needed to maximize the net benefits of LT.
Keywords: clinical decision-making; clinical research/practice; epidemiology; geriatrics; lung transplantation/pulmonology; organ allocation; quality of life (QOL).
© 2016 The American Society of Transplantation and the American Society of Transplant Surgeons.
Conflict of interest statement
The authors of this manuscript have no conflicts of interest to disclose as described by the
Figures
References
-
- Thabut G, Ravaud P, Christie JD, Castier Y, Fournier M, Mal H, et al. Determinants of the Survival Benefit of Lung Transplantation in Patients with Chronic Obstructive Pulmonary Disease. Am J Resp Crit Care Med. 2008;177(10):1156–1163. - PubMed
-
- Yusen RD, Christie JD, Edwards LB, Kucheryavaya AY, Benden C, Dipchand AI, et al. The Registry of the International Society for Heart and Lung Transplantation: thirtieth adult lung and heart-lung transplant report--2013; focus theme: age. J Heart Lung Transplant. 2013;32(10):965–978. - PubMed
-
- Egan TM, Murray S, Bustami RT, Shearon TH, McCullough KP, Edwards LB, et al. Development of the new lung allocation system in the United States. Am J Transplant. 2006;6(5 Pt 2):1212–1227. - PubMed
-
- Hoopes CW, Kukreja J, Golden J, Davenport DL, Diaz-Guzman E, Zwischenberger JB. Extracorporeal membrane oxygenation as a bridge to pulmonary transplantation. J Thorac Cardiovasc Surg. 2013;145(3):862–867. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
