

Prostate Health Index improves multivariable risk prediction of aggressive prostate cancer
- PMID: 27743489
- PMCID: PMC5392379
- DOI: 10.1111/bju.13676
Prostate Health Index improves multivariable risk prediction of aggressive prostate cancer
Abstract
Objective: To examine the use of the Prostate Health Index (PHI) as a continuous variable in multivariable risk assessment for aggressive prostate cancer in a large multicentre US study.
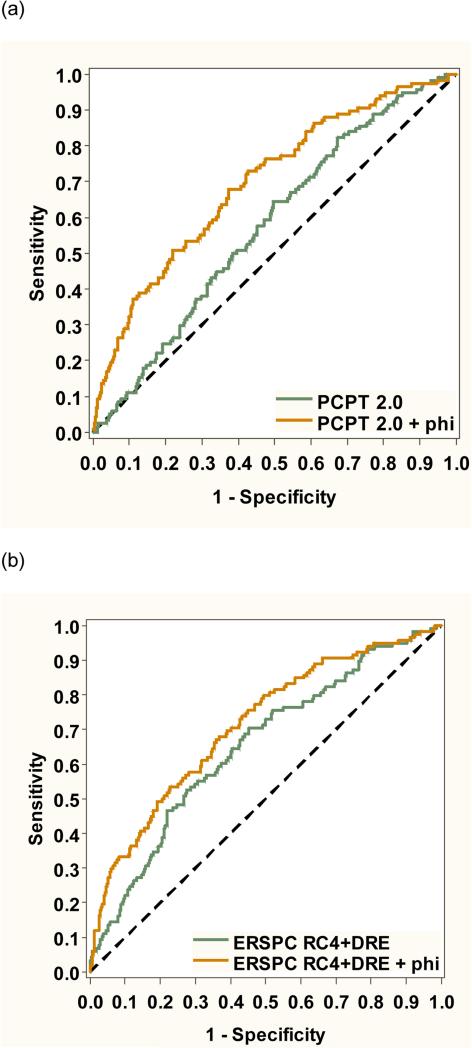
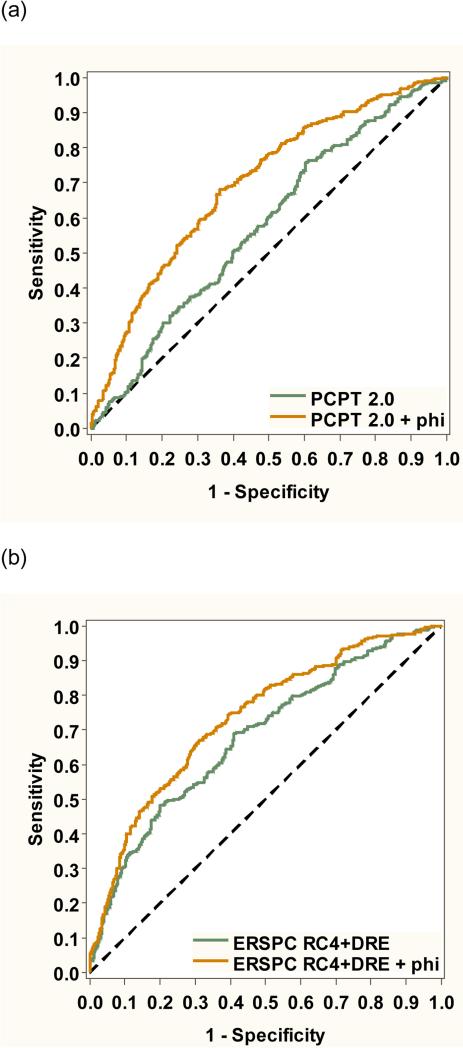
Materials and methods: The study population included 728 men, with prostate-specific antigen (PSA) levels of 2-10 ng/mL and a negative digital rectal examination, enrolled in a prospective, multi-site early detection trial. The primary endpoint was aggressive prostate cancer, defined as biopsy Gleason score ≥7. First, we evaluated whether the addition of PHI improves the performance of currently available risk calculators (the Prostate Cancer Prevention Trial [PCPT] and European Randomised Study of Screening for Prostate Cancer [ERSPC] risk calculators). We also designed and internally validated a new PHI-based multivariable predictive model, and created a nomogram.
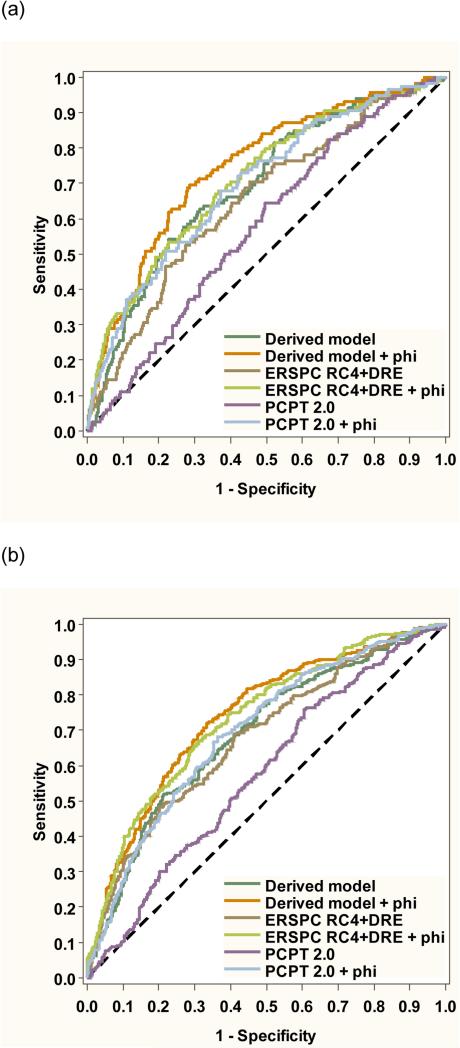
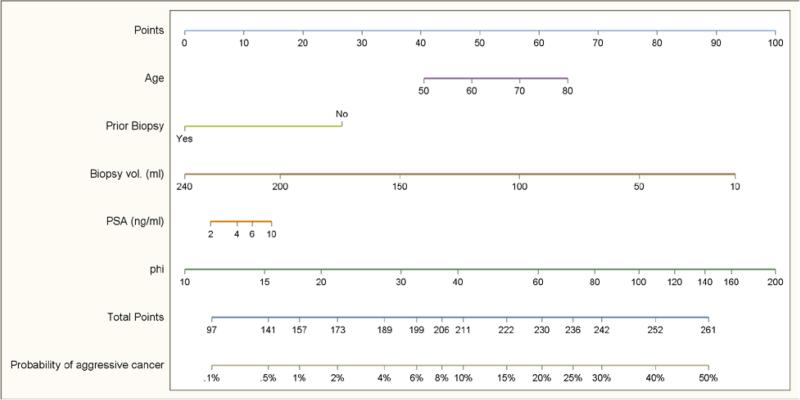
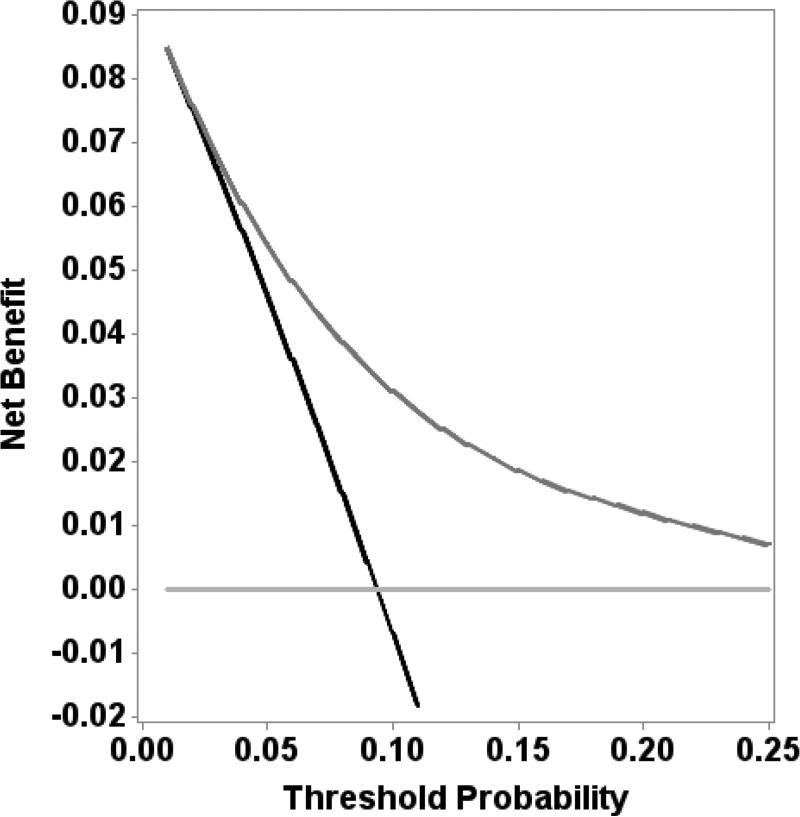
Results: Of 728 men undergoing biopsy, 118 (16.2%) had aggressive prostate cancer. The PHI predicted the risk of aggressive prostate cancer across the spectrum of values. Adding PHI significantly improved the predictive accuracy of the PCPT and ERSPC risk calculators for aggressive disease. A new model was created using age, previous biopsy, prostate volume, PSA and PHI, with an area under the curve of 0.746. The bootstrap-corrected model showed good calibration with observed risk for aggressive prostate cancer and had net benefit on decision-curve analysis.
Conclusion: Using PHI as part of multivariable risk assessment leads to a significant improvement in the detection of aggressive prostate cancer, potentially reducing harms from unnecessary prostate biopsy and overdiagnosis.
Keywords: Prostate Health Index; nomogram; prostate biopsy; prostate cancer; risk assessment.
© 2016 The Authors BJU International © 2016 BJU International Published by John Wiley & Sons Ltd.
Figures
References
-
- Catalona WJ, Partin AW, Sanda MG, Wei JT, Klee GG, Bangma CH, Slawin KM, Marks LS, Loeb S, Broyles DL, Shin SS, Crus AB, Chan DW, Sokoll LJ, Roberts WL, van Schaik RHN, Mizrahi IA. A Multicenter Study of [−2] Pro-Prostate Specific Antigen Combined With Prostate Specific Antigen and Free Prostate Specific Antigen for Prostate Cancer Detection in the 2.0 to 10.0 ng/ml Prostate Specific Antigen Range. J Urol. 2011;185:1650–5. - PMC - PubMed
-
- Hirama H, Sugimoto M, Ito K, Shiraishi T, Kakehi Y. The impact of baseline [−2]proPSA-related indices on the prediction of pathological reclassification at 1 year during active surveillance for low-risk prostate cancer: the Japanese multicenter study cohort. Journal of cancer research and clinical oncology. 2014 Feb;140:257–63. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
