

Factors Influencing the Efficacy of Aerobic Exercise for Improving Fitness and Walking Capacity After Stroke: A Meta-Analysis With Meta-Regression
- PMID: 27744025
- PMCID: PMC5868957
- DOI: 10.1016/j.apmr.2016.08.484
Factors Influencing the Efficacy of Aerobic Exercise for Improving Fitness and Walking Capacity After Stroke: A Meta-Analysis With Meta-Regression
Abstract
Objective: To assess the influence of dosing parameters and patient characteristics on the efficacy of aerobic exercise (AEX) poststroke.
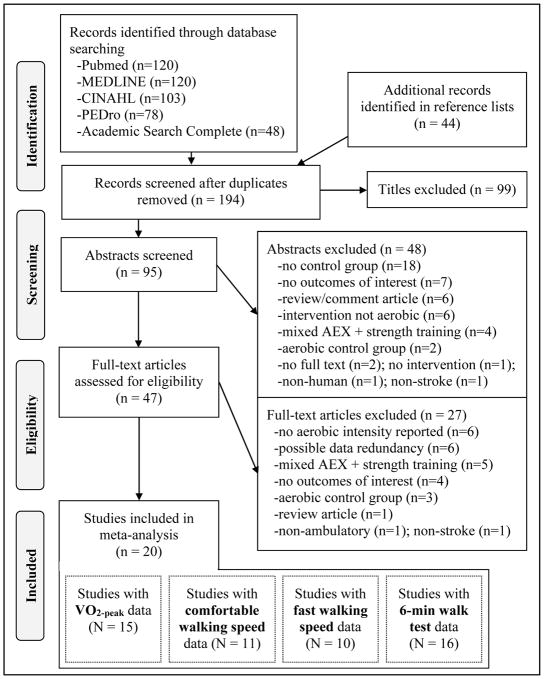
Data sources: A systematic review was conducted using PubMed, MEDLINE, Cumulative Index of Nursing and Allied Health Literature, Physiotherapy Evidence Database, and Academic Search Complete.
Study selection: Studies were selected that compared an AEX group with a nonaerobic control group among ambulatory persons with stroke.
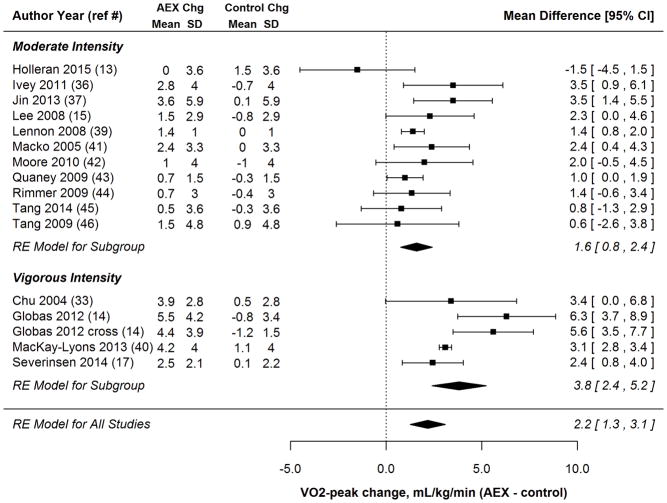
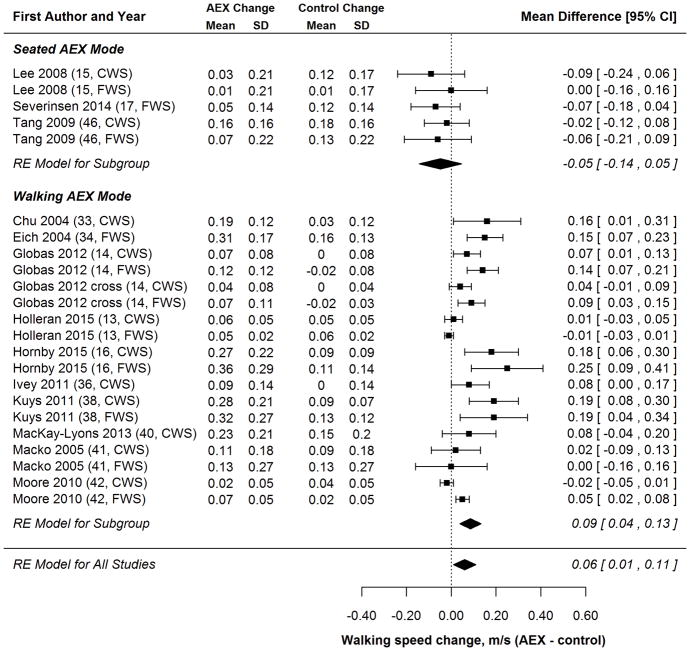
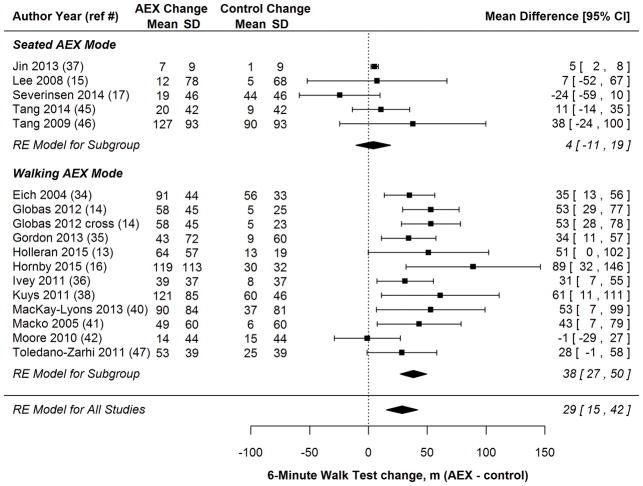
Data extraction: Extracted outcome data included peak oxygen consumption (V˙o2peak) during exercise testing, walking speed, and walking endurance (6-min walk test). Independent variables of interest were AEX mode (seated or walking), AEX intensity (moderate or vigorous), AEX volume (total hours), stroke chronicity, and baseline outcome scores.
Data synthesis: Significant between-study heterogeneity was confirmed for all outcomes. Pooled AEX effect size estimates (AEX group change minus control group change) from random effects models were V˙o2peak, 2.2mL⋅kg-1⋅min-1 (95% confidence interval [CI], 1.3-3.1mL⋅kg-1⋅min-1); walking speed, .06m/s (95% CI, .01-.11m/s); and 6-minute walk test distance, 29m (95% CI, 15-42m). In meta-regression, larger V˙o2peak effect sizes were significantly associated with higher AEX intensity and higher baseline V˙o2peak. Larger effect sizes for walking speed and the 6-minute walk test were significantly associated with a walking AEX mode. In contrast, seated AEX did not have a significant effect on walking outcomes.
Conclusions: AEX significantly improves aerobic capacity poststroke, but may need to be task specific to affect walking speed and endurance. Higher AEX intensity is associated with better outcomes. Future randomized studies are needed to confirm these results.
Keywords: Cardiovascular deconditioning; Exercise; Locomotion; Rehabilitation; Stroke.
Copyright © 2016 American Congress of Rehabilitation Medicine. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures

Similar articles
-
Treadmill exercise rehabilitation improves ambulatory function and cardiovascular fitness in patients with chronic stroke: a randomized, controlled trial.Stroke. 2005 Oct;36(10):2206-11. doi: 10.1161/01.STR.0000181076.91805.89. Epub 2005 Sep 8. Stroke. 2005. PMID: 16151035 Clinical Trial.
-
A Home- and Community-Based Physical Activity Program Can Improve the Cardiorespiratory Fitness and Walking Capacity of Stroke Survivors.J Stroke Cerebrovasc Dis. 2016 Oct;25(10):2386-98. doi: 10.1016/j.jstrokecerebrovasdis.2016.06.007. Epub 2016 Jul 1. J Stroke Cerebrovasc Dis. 2016. PMID: 27378733 Clinical Trial.
-
High Intensity Exercise for Walking Competency in Individuals with Stroke: A Systematic Review and Meta-Analysis.J Stroke Cerebrovasc Dis. 2019 Dec;28(12):104414. doi: 10.1016/j.jstrokecerebrovasdis.2019.104414. Epub 2019 Sep 27. J Stroke Cerebrovasc Dis. 2019. PMID: 31570262
-
Effects of a 6-Week Aquatic Treadmill Exercise Program on Cardiorespiratory Fitness and Walking Endurance in Subacute Stroke Patients: A PILOT TRIAL.J Cardiopulm Rehabil Prev. 2018 Sep;38(5):314-319. doi: 10.1097/HCR.0000000000000243. J Cardiopulm Rehabil Prev. 2018. PMID: 28306685 Clinical Trial.
-
Are Aerobic Programs Similar in Design to Cardiac Rehabilitation Beneficial for Survivors of Stroke? A Systematic Review and Meta-Analysis.J Am Heart Assoc. 2019 Aug 20;8(16):e012761. doi: 10.1161/JAHA.119.012761. Epub 2019 Aug 14. J Am Heart Assoc. 2019. PMID: 31409176 Free PMC article.
Cited by
-
An 8-week Forced-rate Aerobic Cycling Program Improves Cardiorespiratory Fitness in Persons With Chronic Stroke: A Randomized Controlled Trial.Arch Phys Med Rehabil. 2024 May;105(5):835-842. doi: 10.1016/j.apmr.2024.01.018. Epub 2024 Feb 11. Arch Phys Med Rehabil. 2024. PMID: 38350494 Free PMC article. Clinical Trial.
-
Enhancing Neuroplasticity in the Chronic Phase After Stroke: Effects of a Soft Robotic Exosuit on Training Intensity and Brain-Derived Neurotrophic Factor.IEEE Open J Eng Med Biol. 2023 Sep 8;4:284-291. doi: 10.1109/OJEMB.2023.3313396. eCollection 2023. IEEE Open J Eng Med Biol. 2023. PMID: 38196979 Free PMC article.
-
Enhancing Heart Rate-Based Estimation of Energy Expenditure and Exercise Intensity in Patients Post Stroke.Bioengineering (Basel). 2024 Dec 10;11(12):1250. doi: 10.3390/bioengineering11121250. Bioengineering (Basel). 2024. PMID: 39768068 Free PMC article.
-
Co-Designed Cardiac Rehabilitation for the Secondary Prevention of Stroke (CARESS): A Pilot Program Evaluation.Healthcare (Basel). 2024 Apr 3;12(7):776. doi: 10.3390/healthcare12070776. Healthcare (Basel). 2024. PMID: 38610198 Free PMC article.
-
A Comparison of Three Common Rehabilitation Interventions Used to Improve Cardiovascular Fitness after Stroke: An Overview of the Literature.Biomed Res Int. 2023 Apr 11;2023:4350851. doi: 10.1155/2023/4350851. eCollection 2023. Biomed Res Int. 2023. PMID: 37082188 Free PMC article. Review.
References
-
- Mayo NE, Wood-Dauphinee S, Cote R, Durcan L, Carlton J. Activity, participation, and quality of life 6 months poststroke. Arch Phys Med Rehabil. 2002;83(8):1035–1042. - PubMed
-
- Jorgensen HS, Nakayama H, Raaschou HO, Vive-Larsen J, Stoier M, Olsen TS. Outcome and time course of recovery in stroke. part II: Time course of recovery. The Copenhagen Stroke Study. Arch Phys Med Rehabil. 1995;76(5):406–412. - PubMed
-
- Hill K, Ellis P, Bernhardt J, Maggs P, Hull S. Balance and mobility outcomes for stroke patients: A comprehensive review. Aust J Physiother. 1997;43:173–80. - PubMed
-
- Flansbjer UB, Downham D, Lexell J. Knee muscle strength, gait performance, and perceived participation after stroke. Arch Phys Med Rehabil. 2006;87(7):974–980. - PubMed
-
- Eng JJ, Chu KS, Dawson AS, Kim CM, Hepburn KE. Functional walk tests in individuals with stroke: Relation to perceived exertion and myocardial exertion. Stroke. 2002;33(3):756–761. - PubMed
Studies Excluded After Full Text Review
-
- Bateman A, Culpan FJ, Pickering AD, Powell JH, Scott OM, Greenwood RJ. The effect of aerobic training on rehabilitation outcomes after recent severe brain injury: A randomized controlled evaluation. Arch Phys Med Rehabil. 2001;82(2):174–182. - PubMed
-
- Chang WH, Kim MS, Huh JP, Lee PK, Kim YH. Effects of robot-assisted gait training on cardiopulmonary fitness in subacute stroke patients: A randomized controlled study. Neurorehabil Neural Repair. 2012;26(4):318–324. - PubMed
-
- Dean CM, Richards CL, Malouin F. Task-related circuit training improves performance of locomotor tasks in chronic stroke: A randomized, controlled pilot trial. Arch Phys Med Rehabil. 2000;81(4):409–417. - PubMed
-
- Hesse S, Eich HJ, Mach H, Parchmann H, Werner C. Aerobic treadmill training plus physiotherapy improves walking speed and capacity in subacute, moderately affected patients after stroke. Neurologie und Rehabilitation. 2005;11(1):7–12.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
