Short-term Effects of Ambient Air Pollution on Emergency Department Visits for Asthma: An Assessment of Effect Modification by Prior Allergic Disease History
- PMID: 27744674
- PMCID: PMC5066424
- DOI: 10.3961/jpmph.16.038
Short-term Effects of Ambient Air Pollution on Emergency Department Visits for Asthma: An Assessment of Effect Modification by Prior Allergic Disease History
Abstract
Objectives: The goal of this study was to investigate the short-term effect of ambient air pollution on emergency department (ED) visits in Seoul for asthma according to patients' prior history of allergic diseases.
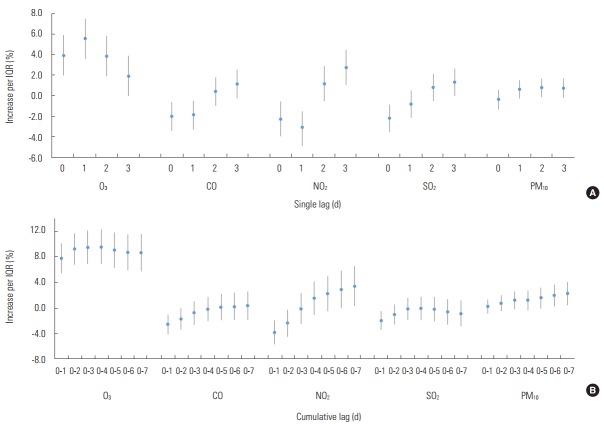
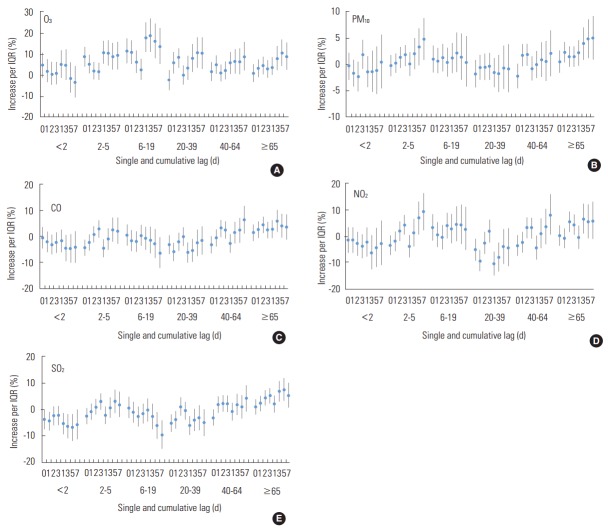
Methods: Data on ED visits from 2005 to 2009 were obtained from the Health Insurance Review and Assessment Service. To evaluate the risk of ED visits for asthma related to ambient air pollutants (carbon monoxide [CO], nitrogen dioxide [NO2], ozone [O3], sulfur dioxide [SO2], and particulate matter with an aerodynamic diameter <10 μm [PM10]), a generalized additive model with a Poisson distribution was used; a single-lag model and a cumulative-effect model (average concentration over the previous 1-7 days) were also explored. The percent increase and 95% confidence interval (CI) were calculated for each interquartile range (IQR) increment in the concentration of each air pollutant. Subgroup analyses were done by age, gender, the presence of allergic disease, and season.
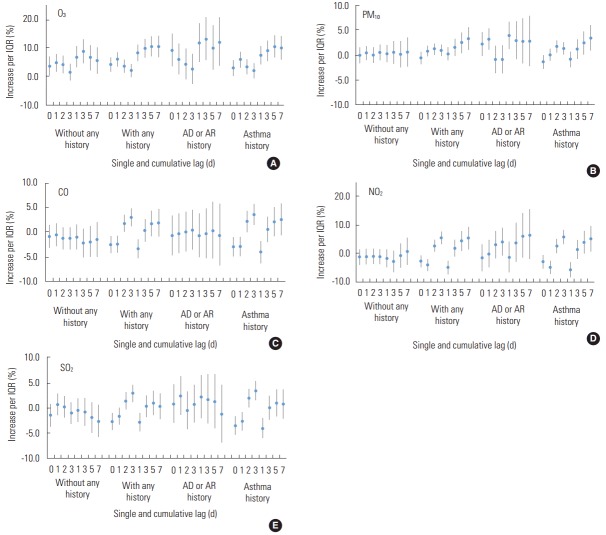
Results: A total of 33 751 asthma attack cases were observed during the study period. The strongest association was a 9.6% increase (95% CI, 6.9% to 12.3%) in the risk of ED visits for asthma per IQR increase in O3 concentration. IQR changes in NO2 and PM10 concentrations were also significantly associated with ED visits in the cumulative lag 7 model. Among patients with a prior history of allergic rhinitis or atopic dermatitis, the risk of ED visits for asthma per IQR increase in PM10 concentration was higher (3.9%; 95% CI, 1.2% to 6.7%) than in patients with no such history.
Conclusions: Ambient air pollutants were positively associated with ED visits for asthma, especially among subjects with a prior history of allergic rhinitis or atopic dermatitis.
Keywords: Air pollution; Asthma; Effect modifier; Emergencies; Korea; Time series analysis.
Conflict of interest statement
The authors have no conflicts of interest associated with the material presented in this paper.
Figures

References
-
- Oh IH, Yoon SJ, Kim EJ. The burden of disease in Korea. J Korean Med Assoc. 2011;54(6):646–652. (Korean)
-
- OECD Health at a glance 2013: OECD indicators. [cited 2016 Sep 16]. Available from: http://apps.who.int/medicinedocs/documents/s21725en/s21725en.pdf.
-
- Korean Academy of Asthma, Allergy and Clinical Immunology. Korean Academy of Pediatric Allergy and Respiratory Disease. National Strategic Coordinating Center for Clinical Research Korean guideline for asthma. 2015 [cited 2016 Sep 16]. Available from: http://www.allergy.or.kr/file/150527_01.pdf.
-
- Kim SY, Jung JY, Park MS, Kang YA, Kim EY, Kim SK, et al. Increased prevalence of self-reported asthma among Korean adults: an analysis of KNHANES I and IV data. Lung. 2013;191(3):281–288. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical