

Carboplatin and pemetrexed with or without pembrolizumab for advanced, non-squamous non-small-cell lung cancer: a randomised, phase 2 cohort of the open-label KEYNOTE-021 study
- PMID: 27745820
- PMCID: PMC6886237
- DOI: 10.1016/S1470-2045(16)30498-3
Carboplatin and pemetrexed with or without pembrolizumab for advanced, non-squamous non-small-cell lung cancer: a randomised, phase 2 cohort of the open-label KEYNOTE-021 study
Abstract
Background: Limited evidence exists to show that adding a third agent to platinum-doublet chemotherapy improves efficacy in the first-line advanced non-small-cell lung cancer (NSCLC) setting. The anti-PD-1 antibody pembrolizumab has shown efficacy as monotherapy in patients with advanced NSCLC and has a non-overlapping toxicity profile with chemotherapy. We assessed whether the addition of pembrolizumab to platinum-doublet chemotherapy improves efficacy in patients with advanced non-squamous NSCLC.
Methods: In this randomised, open-label, phase 2 cohort of a multicohort study (KEYNOTE-021), patients were enrolled at 26 medical centres in the USA and Taiwan. Patients with chemotherapy-naive, stage IIIB or IV, non-squamous NSCLC without targetable EGFR or ALK genetic aberrations were randomly assigned (1:1) in blocks of four stratified by PD-L1 tumour proportion score (<1% vs ≥1%) using an interactive voice-response system to 4 cycles of pembrolizumab 200 mg plus carboplatin area under curve 5 mg/mL per min and pemetrexed 500 mg/m2 every 3 weeks followed by pembrolizumab for 24 months and indefinite pemetrexed maintenance therapy or to 4 cycles of carboplatin and pemetrexed alone followed by indefinite pemetrexed maintenance therapy. The primary endpoint was the proportion of patients who achieved an objective response, defined as the percentage of patients with radiologically confirmed complete or partial response according to Response Evaluation Criteria in Solid Tumors version 1.1 assessed by masked, independent central review, in the intention-to-treat population, defined as all patients who were allocated to study treatment. Significance threshold was p<0·025 (one sided). Safety was assessed in the as-treated population, defined as all patients who received at least one dose of the assigned study treatment. This trial, which is closed for enrolment but continuing for follow-up, is registered with ClinicalTrials.gov, number NCT02039674.
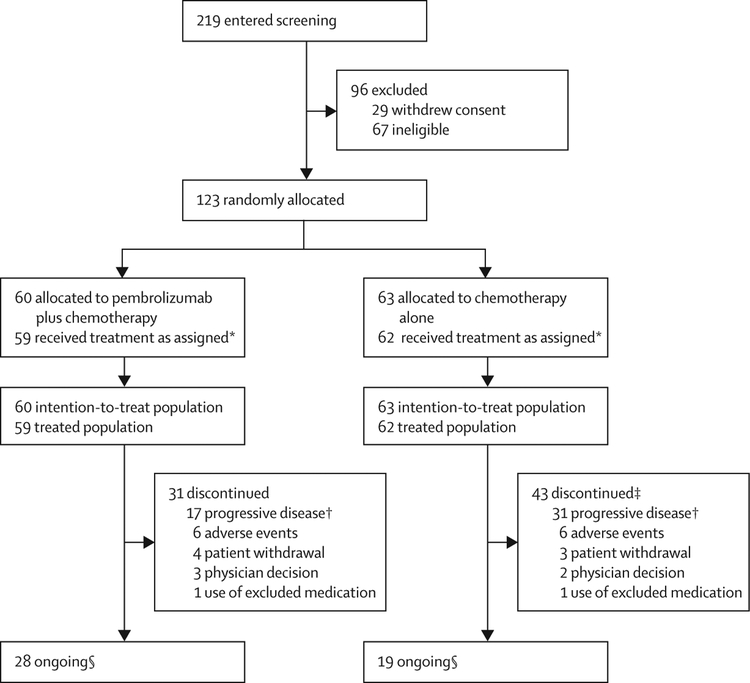
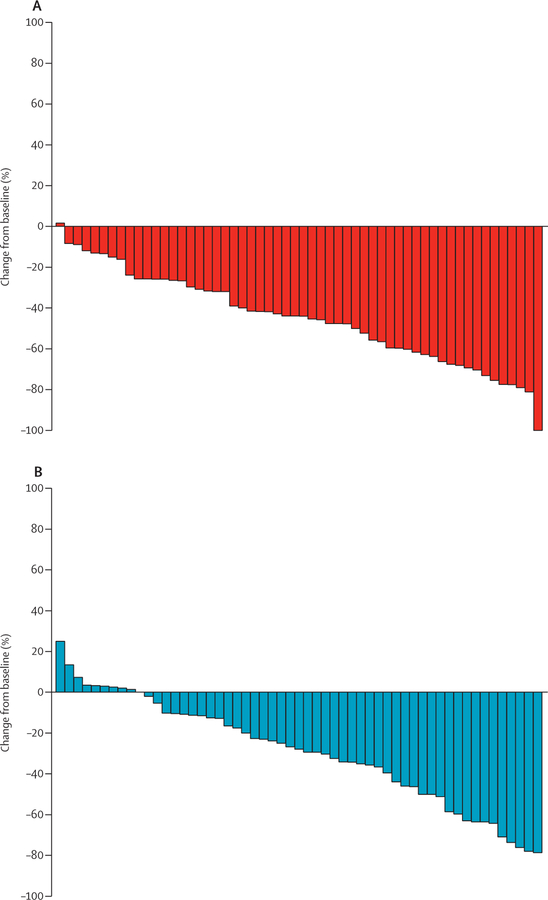
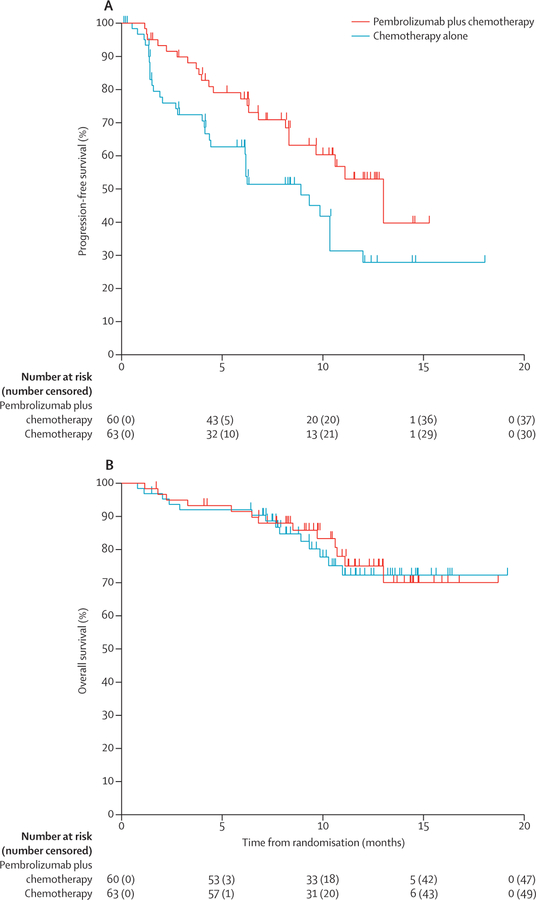
Findings: Between Nov 25, 2014, and Jan 25, 2016, 123 patients were enrolled; 60 were randomly assigned to the pembrolizumab plus chemotherapy group and 63 to the chemotherapy alone group. 33 (55%; 95% CI 42-68) of 60 patients in the pembrolizumab plus chemotherapy group achieved an objective response compared with 18 (29%; 18-41) of 63 patients in the chemotherapy alone group (estimated treatment difference 26% [95% CI 9-42%]; p=0·0016). The incidence of grade 3 or worse treatment-related adverse events was similar between groups (23 [39%] of 59 patients in the pembrolizumab plus chemotherapy group and 16 [26%] of 62 in the chemotherapy alone group). The most common grade 3 or worse treatment-related adverse events in the pembrolizumab plus chemotherapy group were anaemia (seven [12%] of 59) and decreased neutrophil count (three [5%]); an additional six events each occurred in two (3%) for acute kidney injury, decreased lymphocyte count, fatigue, neutropenia, and sepsis, and thrombocytopenia. In the chemotherapy alone group, the most common grade 3 or worse events were anaemia (nine [15%] of 62) and decreased neutrophil count, pancytopenia, and thrombocytopenia (two [3%] each). One (2%) of 59 patients in the pembrolizumab plus chemotherapy group experienced treatment-related death because of sepsis compared with two (3%) of 62 patients in the chemotherapy group: one because of sepsis and one because of pancytopenia.
Interpretation: Combination of pembrolizumab, carboplatin, and pemetrexed could be an effective and tolerable first-line treatment option for patients with advanced non-squamous NSCLC. This finding is being further explored in an ongoing international, randomised, double-blind, phase 3 study.
Funding: Merck & Co.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Diminished but not dead: chemotherapy for the treatment of NSCLC.Lancet Oncol. 2016 Nov;17(11):1464-1465. doi: 10.1016/S1470-2045(16)30524-1. Lancet Oncol. 2016. PMID: 27819227 No abstract available.
References
-
- Sandler A, Gray R, Perry MC, et al. Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer. N Engl J Med 2006; 355: 2542–50. - PubMed
-
- Garon EB, Rizvi NA, Hui R, et al. Pembrolizumab for the treatment of non-small-cell lung cancer. N Engl J Med 2015; 372: 2018–28. - PubMed
-
- Herbst RS, Baas P, Kim DW, et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): a randomised controlled trial. Lancet 2016; 387: 1540–50. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
