

Pectus excavatum from a pediatric surgeon's perspective
- PMID: 27747183
- PMCID: PMC5056929
- DOI: 10.21037/acs.2016.06.04
Pectus excavatum from a pediatric surgeon's perspective
Abstract
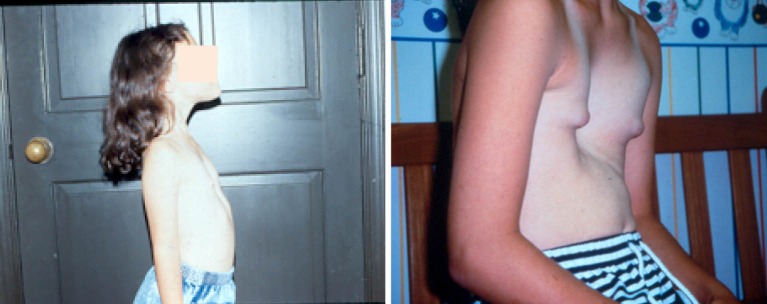
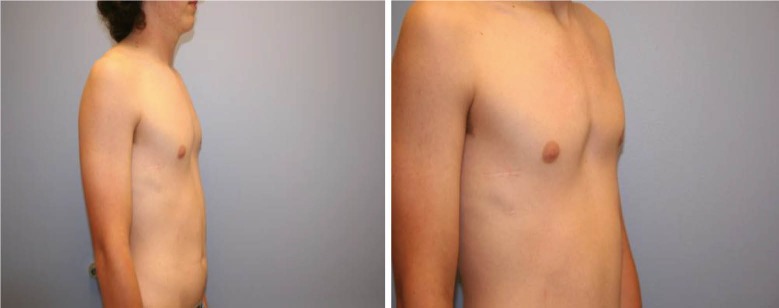
Historically, pectus excavatum (PE) was reported to be congenital, but in our experience only 22% are noticed in the first decade of life. Thus far, genetic studies support an autosomal recessive heritability, which coincides with only 40% of our patients having some positive family history, but is also contradictory given a constant sex ratio of 4:1 in favor of males. This inconsistency may be explained by the effect of more than one pectus disease-associated allele. Once the deformity is noticed, it tends to progress slowly until puberty, when rapid progression is often seen. We recommend surgical repair at around 12-14 years of age since the chest wall is still typically flexible and because this allows us to keep the bar in place as the patient progresses through puberty which may help decrease growth-related recurrences. Patients with mild to moderate PE are treated with therapeutic deep breathing, posturing, and aerobic exercises, and in appropriately selected patients, the vacuum bell may also be offered. Patients that have severe symptomatic PE are offered Minimally Invasive Repair of Pectus Excavatum (MIRPE). The surgical technique in children is similar to that of adults, except for the higher forces involved that often necessitate sternal elevation and more involved stabilization strategies. Postoperative management includes pain control, deep breathing, and early ambulation. Exercise restriction is mandatory for the first six weeks with slow resumption of normal activity after 12 weeks.
Keywords: Pediatric pectus excavatum; conservative management; genetics; minimally invasive repair; post-operative management.
Conflict of interest statement
Dr. Nuss has consultation and a royalty agreement with Zimmer Biomet. Dr. Kelly and Dr. Obermeyer have consultation agreements with Biomet Zimmer Biomet.
Figures


References
-
- Brown AL. Pectus Excavatum (Funnel Chest). J Thorac Surg 1939;9:164.
-
- Welch KJ. Satisfactory surgical correction of pectus excavatum deformity in childhood; a limited opportunity. J Thorac Surg 1958;36:697-713. - PubMed
-
- Welch KJ, Randolph JG, Ravitch MM, et al. (eds.) Pediatric Surgery 4th Edition. Chicago: Year Book 1986;57:574.
-
- Welch KJ, Shamberger RC. Chest Wall Deformities in General Thoracic Surgery, 3rd Edition, Ed. By Shields TW, 1989:515-23.
LinkOut - more resources
Full Text Sources
Other Literature Sources