

Cardiovascular diseases related to ionizing radiation: The risk of low-dose exposure (Review)
- PMID: 27748824
- PMCID: PMC5117755
- DOI: 10.3892/ijmm.2016.2777
Cardiovascular diseases related to ionizing radiation: The risk of low-dose exposure (Review)
Abstract
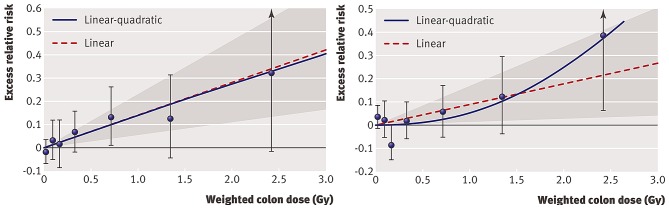
Traditionally, non-cancer diseases are not considered as health risks following exposure to low doses of ionizing radiation. Indeed, non-cancer diseases are classified as deterministic tissue reactions, which are characterized by a threshold dose. It is judged that below an absorbed dose of 100 mGy, no clinically relevant tissue damage occurs, forming the basis for the current radiation protection system concerning non-cancer effects. Recent epidemiological findings point, however, to an excess risk of non-cancer diseases following exposure to lower doses of ionizing radiation than was previously thought. The evidence is the most sound for cardiovascular disease (CVD) and cataract. Due to limited statistical power, the dose-risk relationship is undetermined below 0.5 Gy; however, if this relationship proves to be without a threshold, it may have considerable impact on current low‑dose health risk estimates. In this review, we describe the CVD risk related to low doses of ionizing radiation, the clinical manifestation and the pathology of radiation-induced CVD, as well as the importance of the endothelium models in CVD research as a way forward to complement the epidemiological data with the underlying biological and molecular mechanisms.
Figures
References
-
- Stewart JR, Fajardo LF. Radiation-induced heart disease. Clinical and experimental aspects. Radiol Clin North Am. 1971;9:511–531. - PubMed
-
- Clarke M, Collins R, Darby S, Davies C, Elphinstone P, Evans V, Godwin J, Gray R, Hicks C, James S, et al. Early Breast Cancer Trialists' Collaborative Group (EBCTCG) Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: An overview of the randomised trials. Lancet. 2005;366:2087–2106. doi: 10.1016/S0140-6736(05)67887-7. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
