

Balanced Crystalloids versus Saline in the Intensive Care Unit. The SALT Randomized Trial
- PMID: 27749094
- PMCID: PMC5443900
- DOI: 10.1164/rccm.201607-1345OC
Balanced Crystalloids versus Saline in the Intensive Care Unit. The SALT Randomized Trial
Abstract
Rationale: Saline is the intravenous fluid most commonly administered to critically ill adults, but it may be associated with acute kidney injury and death. Whether use of balanced crystalloids rather than saline affects patient outcomes remains unknown.
Objectives: To pilot a cluster-randomized, multiple-crossover trial using software tools within the electronic health record to compare saline to balanced crystalloids.
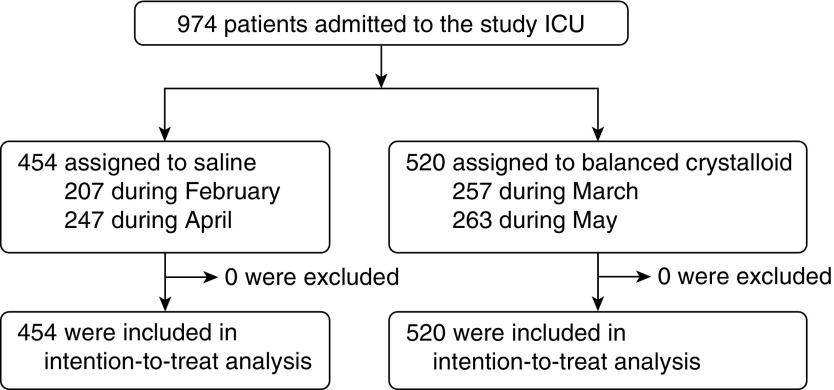
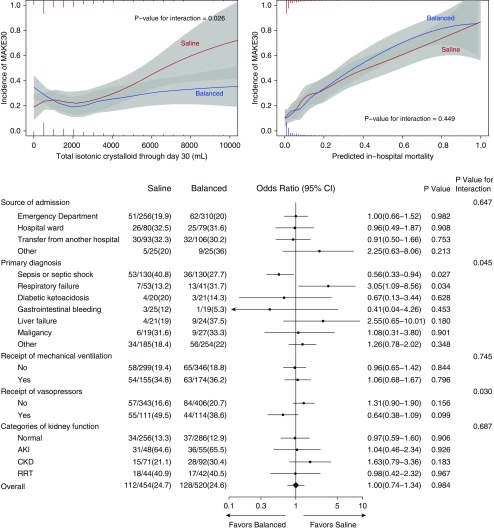
Methods: This was a cluster-randomized, multiple-crossover trial among 974 adults admitted to a tertiary medical intensive care unit from February 3, 2015 to May 31, 2015. The intravenous crystalloid used in the unit alternated monthly between saline (0.9% sodium chloride) and balanced crystalloids (lactated Ringer's solution or Plasma-Lyte A). Enrollment, fluid delivery, and data collection were performed using software tools within the electronic health record. The primary outcome was the difference between study groups in the proportion of isotonic crystalloid administered that was saline. The secondary outcome was major adverse kidney events within 30 days (MAKE30), a composite of death, dialysis, or persistent renal dysfunction.
Measurements and main results: Patients assigned to saline (n = 454) and balanced crystalloids (n = 520) were similar at baseline and received similar volumes of crystalloid by 30 days (median [interquartile range]: 1,424 ml [500-3,377] vs. 1,617 ml [500-3,628]; P = 0.40). Saline made up a larger proportion of the isotonic crystalloid given in the saline group than in the balanced crystalloid group (91% vs. 21%; P < 0.001). MAKE30 did not differ between groups (24.7% vs. 24.6%; P = 0.98).
Conclusions: An electronic health record-embedded, cluster-randomized, multiple-crossover trial comparing saline with balanced crystalloids can produce well-balanced study groups and separation in crystalloid receipt. Clinical trial registered with www.clinicaltrials.gov (NCT 02345486).
Trial registration: ClinicalTrials.gov NCT02345486.
Keywords: acute kidney injury; critical illness; crystalloid; intravenous fluid; saline.
Figures

Comment in
-
Learning Health Care System: Pragmatic Comparison of Crystalloid Choice in a Medical Intensive Care Unit.Am J Respir Crit Care Med. 2017 May 15;195(10):1287-1289. doi: 10.1164/rccm.201610-2093ED. Am J Respir Crit Care Med. 2017. PMID: 28504605 No abstract available.
-
We Do Not Appreciate SALT.Am J Respir Crit Care Med. 2018 May 15;197(10):1361. doi: 10.1164/rccm.201709-1874LE. Am J Respir Crit Care Med. 2018. PMID: 29253347 No abstract available.
-
Reply to Vincent and De Backer: We Do Not Appreciate SALT.Am J Respir Crit Care Med. 2018 May 15;197(10):1362. doi: 10.1164/rccm.201803-0392LE. Am J Respir Crit Care Med. 2018. PMID: 29509507 Free PMC article. No abstract available.
References
-
- Myburgh JA, Mythen MG. Resuscitation fluids. N Engl J Med. 2013;369:1243–1251. - PubMed
-
- Yunos NM, Bellomo R, Hegarty C, Story D, Ho L, Bailey M. Association between a chloride-liberal vs chloride-restrictive intravenous fluid administration strategy and kidney injury in critically ill adults. JAMA. 2012;308:1566–1572. - PubMed
-
- Shaw AD, Bagshaw SM, Goldstein SL, Scherer LA, Duan M, Schermer CR, Kellum JA. Major complications, mortality, and resource utilization after open abdominal surgery: 0.9% saline compared to Plasma-Lyte. Ann Surg. 2012;255:821–829. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
