

Pediatric Type 1 Diabetes: Reducing Admission Rates for Diabetes Ketoacidosis
- PMID: 27749721
- PMCID: PMC5054972
- DOI: 10.1097/QMH.0000000000000109
Pediatric Type 1 Diabetes: Reducing Admission Rates for Diabetes Ketoacidosis
Abstract
Background: Diabetes ketoacidosis (DKA) is a life-threatening complication of type 1 diabetes mellitus (T1DM). Reducing DKA admissions in children with T1DM requires a coordinated, comprehensive management plan. We aimed to decrease DKA admissions, 30-day readmissions, and length of stay (LOS) for DKA admissions.
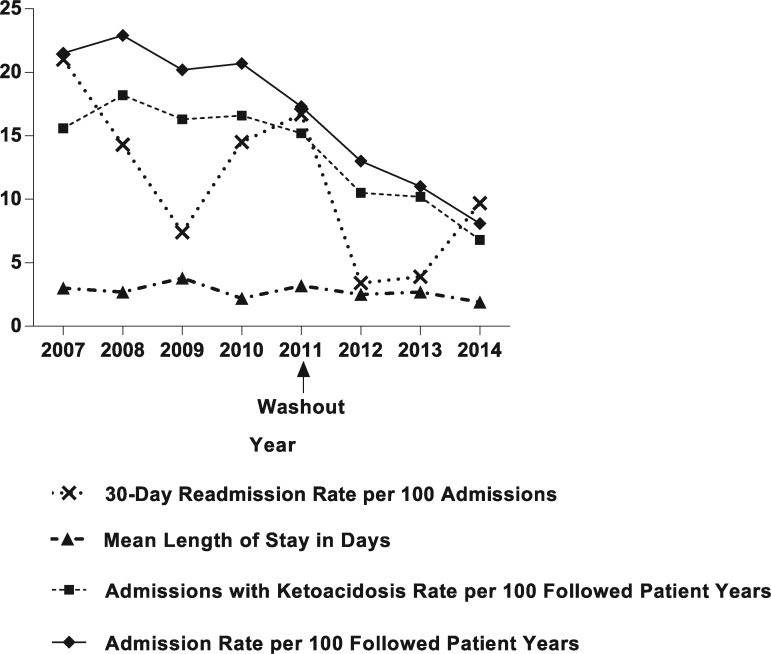
Methods: A multipronged intervention was designed in 2011 to reach all patients: (1) increase insulin pump use and basal-bolus regimen versus sliding scales, (2) transform educational program, (3) increased access to medical providers, and (4) support for patients and families. A before-after study was conducted comparing performance outcomes in years 2007-2010 (preintervention) to 2012-2014 (postintervention) using administrative data and Wilcoxon rank sum and Fischer exact tests.
Results: DKA admissions decreased by 44% postintervention (16.7 vs 9.3 per 100 followed patient-years; P = .006), unique patient 30-day readmissions decreased from 20% to 5% postintervention (P = .001), and median LOS significantly decreased postintervention (P < .0001). Although not an original goal of the study, median hemoglobin A1C of a subset of the population transitioned from sliding scale decreased, 10.3% to 8.9% (P < .02).
Conclusions: When clinical and widespread program interventions were used, significant reductions in DKA hospitalizations, 30-day readmissions, and LOS occurred for pediatric T1DM. Continuous performance improvement efforts are needed for improving DKA outcomes.
Figures
References
-
- Dahlquist G, Mustonen L. Analysis of 20 years of prospective registration of childhood onset diabetes time trends and birth cohort effects. Swedish Childhood Diabetes Study Group. Acta Paediatr. 2000;89(10):1231–1237. - PubMed
-
- Giannini C, Mohn A, Chiarelli F. Technology and the issue of cost/benefit in diabetes. Diabetes Metab Res Rev. 2009;25(suppl 1)(1):S34–S44. - PubMed
-
- Ying AK, Lairson DR, Giardino AP, et al. Predictors of direct costs of diabetes care in pediatric patients with type 1 diabetes. Pediatr Diabetes. 2011;12(3 Pt 1):177–182. - PubMed
-
- Bratcher CR, Bello E. Traditional or centralized models of diabetes care: the multidisciplinary diabetes team approach. J Fam Pract. 2011;60(11 suppl):S6–S11. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
