

Hypophysitis Secondary to Cytotoxic T-Lymphocyte-Associated Protein 4 Blockade: Insights into Pathogenesis from an Autopsy Series
- PMID: 27750046
- PMCID: PMC5225294
- DOI: 10.1016/j.ajpath.2016.08.020
Hypophysitis Secondary to Cytotoxic T-Lymphocyte-Associated Protein 4 Blockade: Insights into Pathogenesis from an Autopsy Series
Abstract
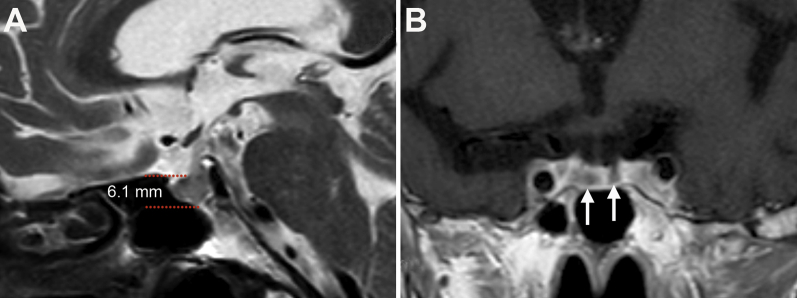
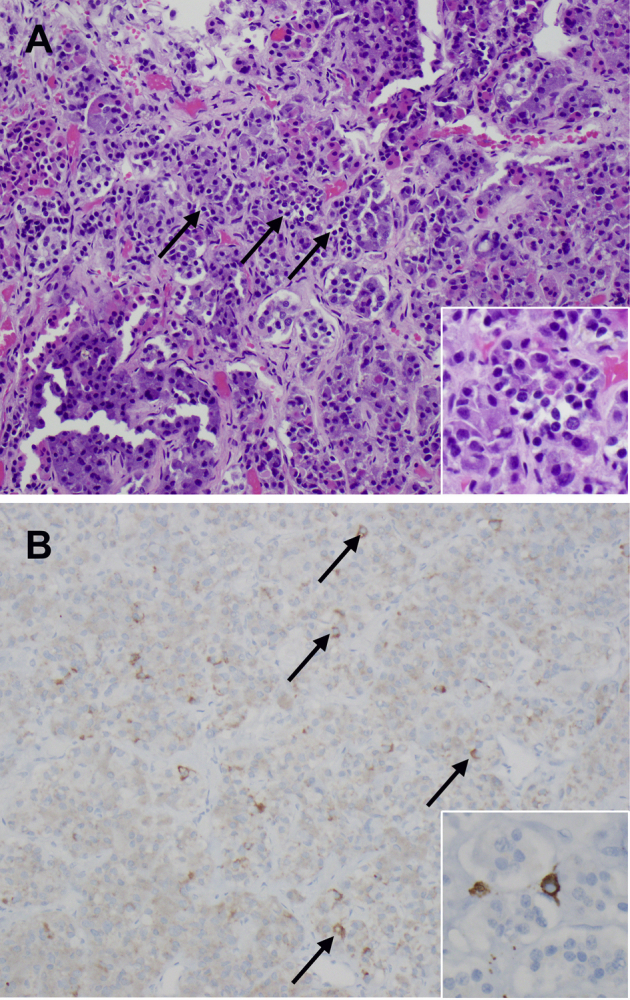
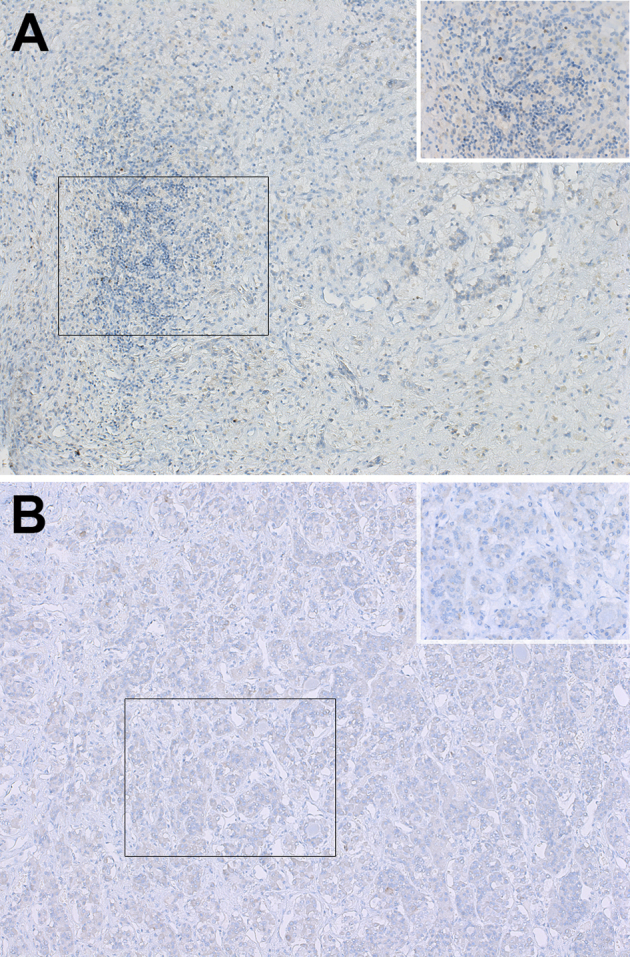
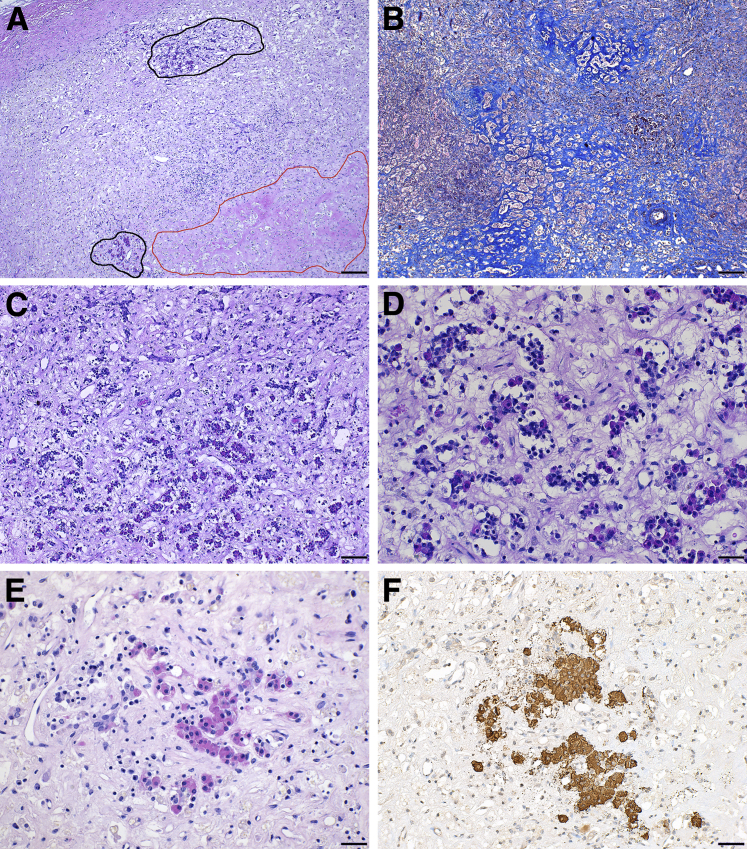
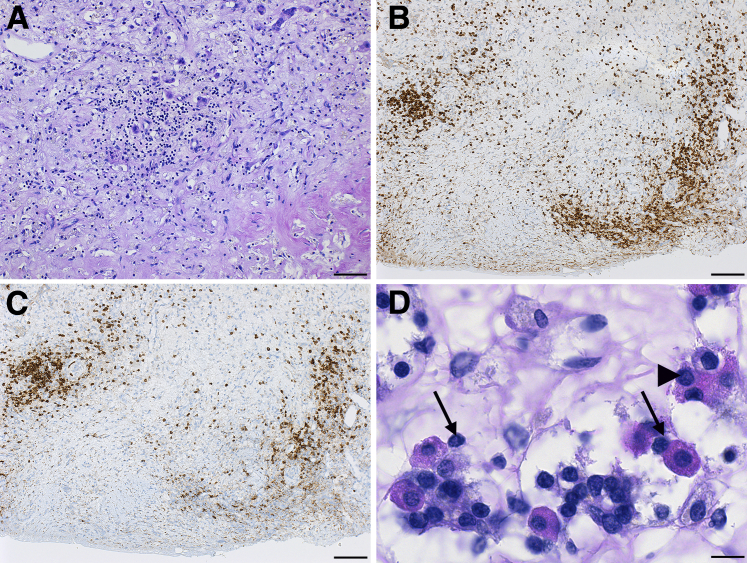
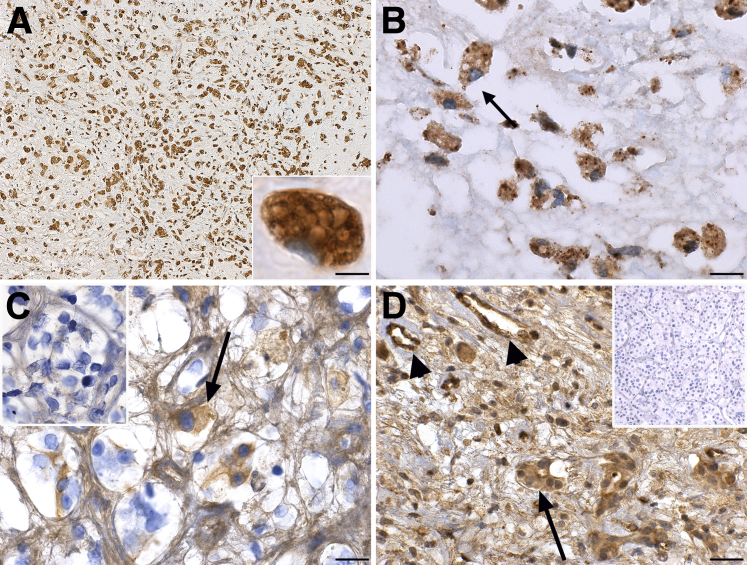
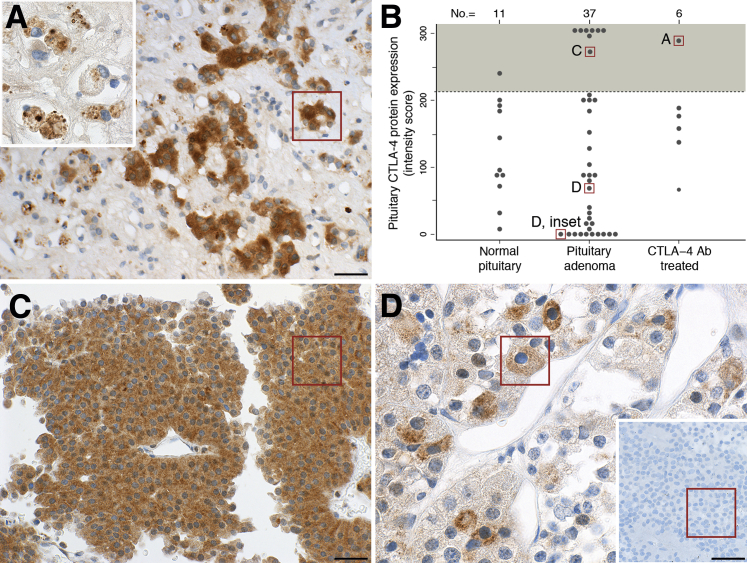
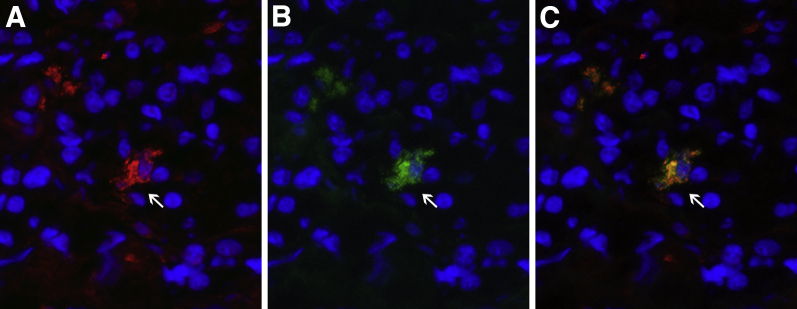
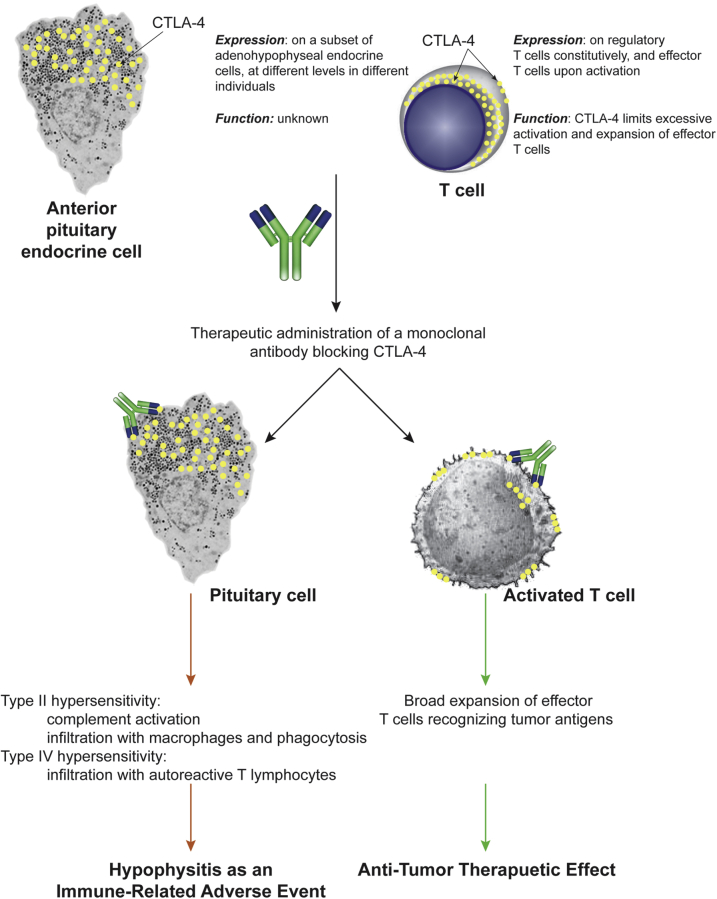
Hypophysitis that develops in cancer patients treated with monoclonal antibodies blocking cytotoxic T-lymphocyte-associated protein 4 (CTLA-4; an inhibitory molecule classically expressed on T cells) is now reported at an incidence of approximately 10%. Its pathogenesis is unknown, in part because no pathologic examination of the pituitary gland has been reported to date. We analyzed at autopsy the pituitary glands of six cancer patients treated with CTLA-4 blockade, one with clinical and pathologic evidence of hypophysitis, one with mild lymphocytic infiltration in the pituitary gland but no clinical signs of hypophysitis, and four with normal pituitary structure and function. CTLA-4 antigen was expressed by pituitary endocrine cells in all patients but at different levels. The highest levels were found in the patient who had clinical and pathologic evidence of severe hypophysitis. This high pituitary CTLA-4 expression was associated with T-cell infiltration and IgG-dependent complement fixation and phagocytosis, immune reactions that induced an extensive destruction of the adenohypophyseal architecture. Pituitary CTLA-4 expression was confirmed in a validation group of 37 surgical pituitary adenomas and 11 normal pituitary glands. The study suggests that administration of CTLA-4 blocking antibodies to patients who express high levels of CTLA-4 antigen in the pituitary can cause an aggressive (necrotizing) form of hypophysitis through type IV (T-cell dependent) and type II (IgG dependent) immune mechanisms.
Copyright © 2016 American Society for Investigative Pathology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Caturegli P., Iwama S. From Japan with love: another tessera in the hypophysitis mosaic. J Clin Endocrinol Metab. 2013;98:1865–1868. - PubMed
-
- Caturegli P., Newschaffer C., Olivi A., Pomper M.G., Burger P.C., Rose N.R. Autoimmune hypophysitis. Endocr Rev. 2005;26:599–614. - PubMed
-
- Deodhare S.S., Bilbao J.M., Kovacs K., Horvath E., Nomikos P., Buchfelder M., Reschke K., Lehnert H. Xanthomatous hypophysitis: a novel entity of obscure etiology. Endocr Pathol. 1999;10:237–241. - PubMed
-
- van der Vliet H.J., Perenboom R.M. Multiple pseudotumors in IgG4-associated multifocal systemic fibrosis. Ann Intern Med. 2004;141:896–897. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
