

The development and validation of the AMPREDICT model for predicting mobility outcome after dysvascular lower extremity amputation
- PMID: 27751738
- PMCID: PMC7521625
- DOI: 10.1016/j.jvs.2016.08.078
The development and validation of the AMPREDICT model for predicting mobility outcome after dysvascular lower extremity amputation
Abstract
Objective: The objective of this study was the development of AMPREDICT-Mobility, a tool to predict the probability of independence in either basic or advanced (iBASIC or iADVANCED) mobility 1 year after dysvascular major lower extremity amputation.
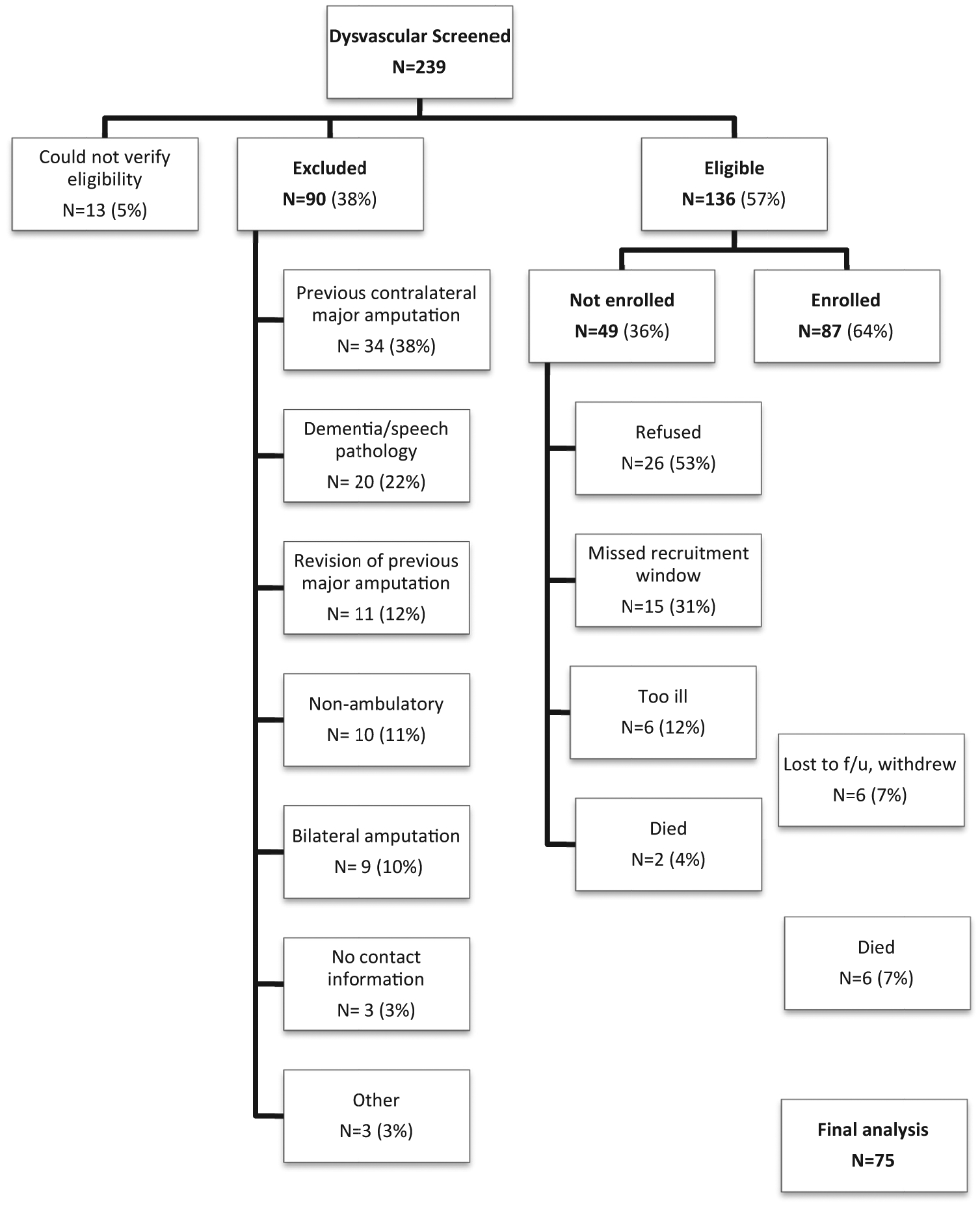
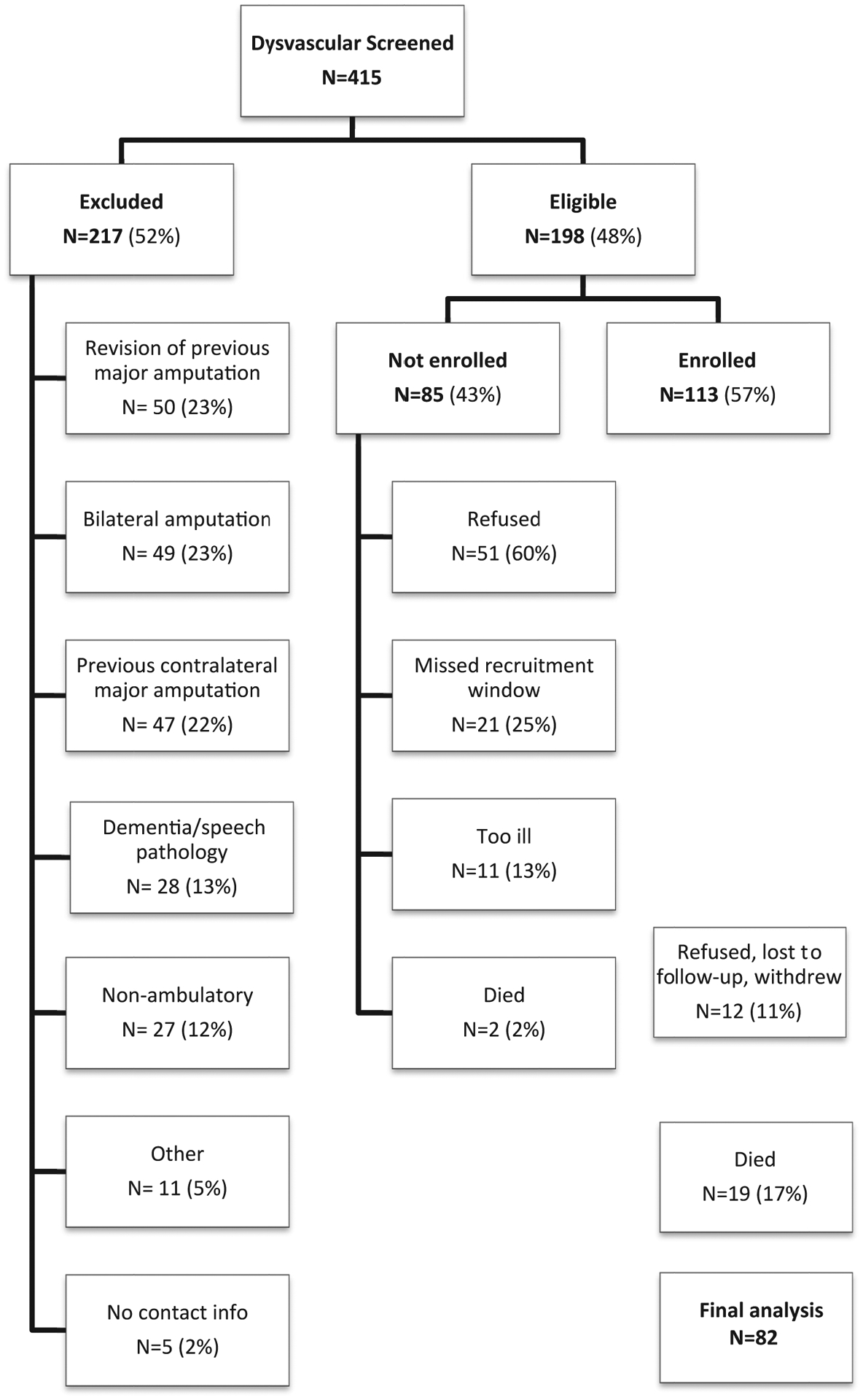
Methods: Two prospective cohort studies during consecutive 4-year periods (2005-2009 and 2010-2014) were conducted at seven medical centers. Multiple demographic and biopsychosocial predictors were collected in the periamputation period among individuals undergoing their first major amputation because of complications of peripheral arterial disease or diabetes. The primary outcomes were iBASIC and iADVANCED mobility, as measured by the Locomotor Capabilities Index. Combined data from both studies were used for model development and internal validation. Backwards stepwise logistic regression was used to develop the final prediction models. The discrimination and calibration of each model were assessed. Internal validity of each model was assessed with bootstrap sampling.
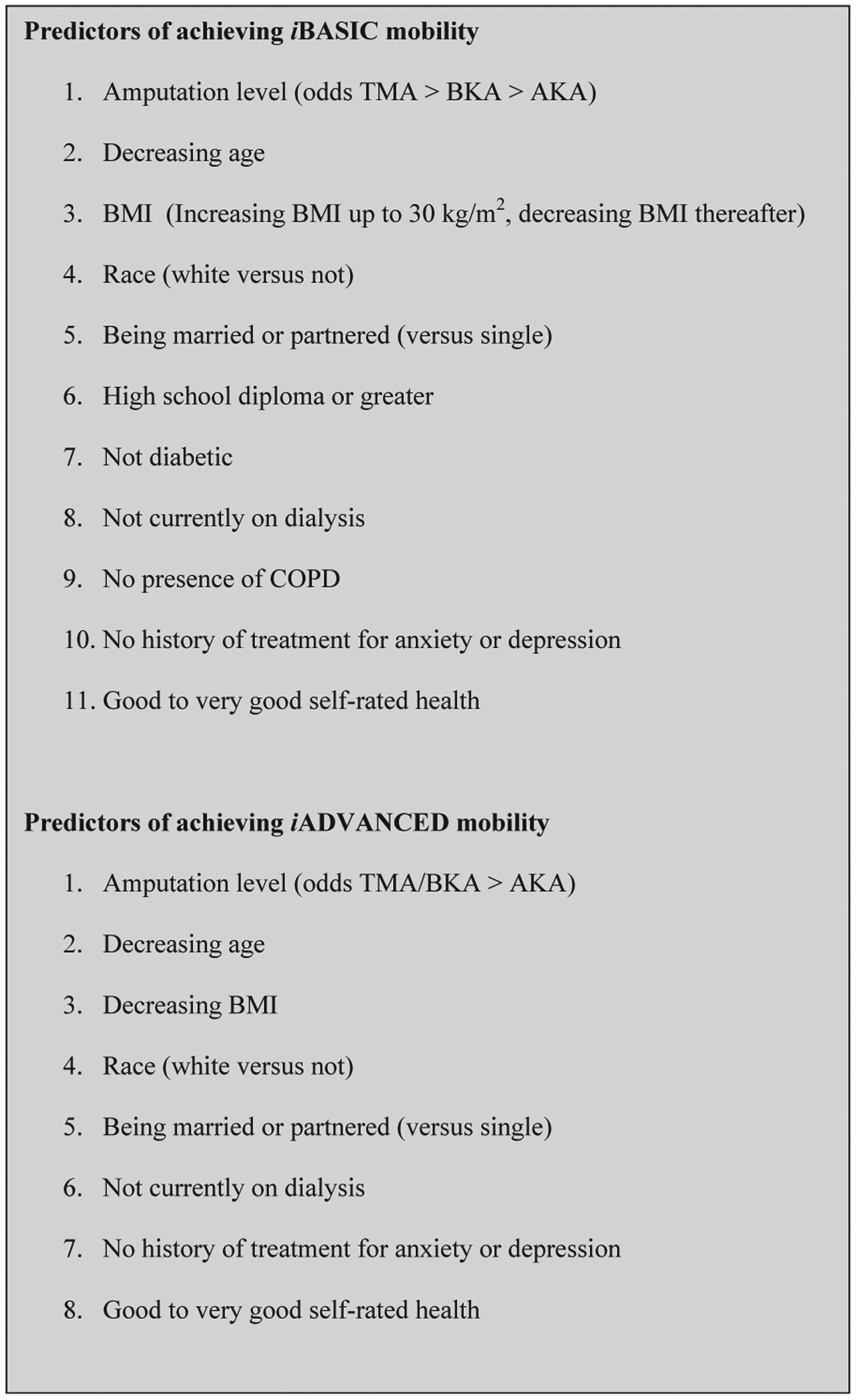
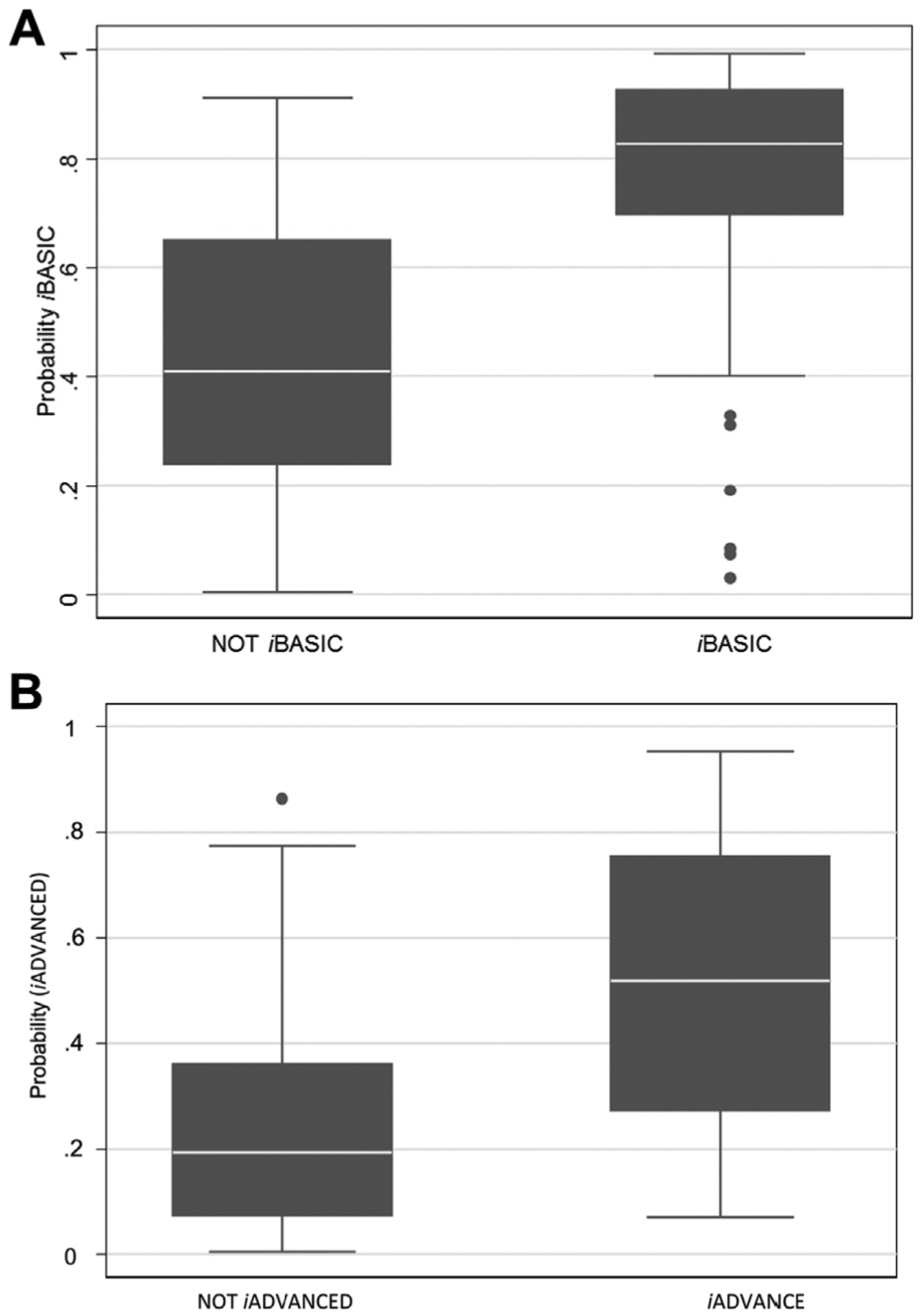
Results: Twelve-month follow-up was reached by 157 of 200 (79%) participants. Among these, 54 (34%) did not achieve iBASIC mobility, 103 (66%) achieved at least iBASIC mobility, and 51 (32%) also achieved iADVANCED mobility. Predictive factors associated with reduced odds of achieving iBASIC mobility were increasing age, chronic obstructive pulmonary disease, dialysis, diabetes, prior history of treatment for depression or anxiety, and very poor to fair self-rated health. Those who were white, were married, and had at least a high-school degree had a higher probability of achieving iBASIC mobility. The odds of achieving iBASIC mobility increased with increasing body mass index up to 30 kg/m2 and decreased with increasing body mass index thereafter. The prediction model of iADVANCED mobility included the same predictors with the exception of diabetes, chronic obstructive pulmonary disease, and education level. Both models showed strong discrimination with C statistics of 0.85 and 0.82, respectively. The mean difference in predicted probabilities for those who did and did not achieve iBASIC and iADVANCED mobility was 33% and 29%, respectively. Tests for calibration and observed vs predicted plots suggested good fit for both models; however, the precision of the estimates of the predicted probabilities was modest. Internal validation through bootstrapping demonstrated some overoptimism of the original model development, with the optimism-adjusted C statistic for iBASIC and iADVANCED mobility being 0.74 and 0.71, respectively, and the discrimination slope 19% and 16%, respectively.
Conclusions: AMPREDICT-Mobility is a user-friendly prediction tool that can inform the patient undergoing a dysvascular amputation and the patient's provider about the probability of independence in either basic or advanced mobility at each major lower extremity amputation level.
Copyright © 2016 Society for Vascular Surgery. All rights reserved.
Conflict of interest statement
Author conflict of interest: none.
The editors and reviewers of this article have no relevant financial relationships to disclose per the JVS policy that requires reviewers to decline review of any manuscript for which they may have a conflict of interest.
Figures
Similar articles
-
Defining successful mobility after lower extremity amputation for complications of peripheral vascular disease and diabetes.J Vasc Surg. 2011 Aug;54(2):412-9. doi: 10.1016/j.jvs.2011.01.046. Epub 2011 Apr 30. J Vasc Surg. 2011. PMID: 21531528 Free PMC article.
-
Ambulation and functional outcome after major lower extremity amputation.J Vasc Surg. 2018 May;67(5):1521-1529. doi: 10.1016/j.jvs.2017.10.051. Epub 2018 Mar 1. J Vasc Surg. 2018. PMID: 29502998
-
The development and validation of a novel outcome measure to quantify mobility in the dysvascular lower extremity amputee: the amputee single item mobility measure.Clin Rehabil. 2016 Sep;30(9):878-89. doi: 10.1177/0269215516644308. Clin Rehabil. 2016. PMID: 27496697 Free PMC article.
-
A Systematic Review and Narrative Synthesis of Risk Prediction Tools Used to Estimate Mortality, Morbidity, and Other Outcomes Following Major Lower Limb Amputation.Eur J Vasc Endovasc Surg. 2021 Jul;62(1):127-135. doi: 10.1016/j.ejvs.2021.02.038. Epub 2021 Apr 24. Eur J Vasc Endovasc Surg. 2021. PMID: 33903018 Free PMC article.
-
Development of Core Outcome Sets for People Undergoing Major Lower Limb Amputation for Complications of Peripheral Vascular Disease.Eur J Vasc Endovasc Surg. 2020 Nov;60(5):730-738. doi: 10.1016/j.ejvs.2020.06.021. Epub 2020 Aug 11. Eur J Vasc Endovasc Surg. 2020. PMID: 32798206
Cited by
-
Understanding the experience of veterans who require lower limb amputation in the veterans health administration.PLoS One. 2022 Mar 18;17(3):e0265620. doi: 10.1371/journal.pone.0265620. eCollection 2022. PLoS One. 2022. PMID: 35303030 Free PMC article.
-
A Prospective Longitudinal Study of Trajectories of Depressive Symptoms After Dysvascular Amputation.Arch Phys Med Rehabil. 2019 Aug;100(8):1426-1433.e1. doi: 10.1016/j.apmr.2018.11.024. Epub 2018 Dec 31. Arch Phys Med Rehabil. 2019. PMID: 30605638 Free PMC article.
-
Long-term risk prediction after major lower limb amputation: 1-year results of the PERCEIVE study.BJS Open. 2024 Jan 3;8(1):zrad135. doi: 10.1093/bjsopen/zrad135. BJS Open. 2024. PMID: 38266124 Free PMC article.
-
Within-subject effects of standardized prosthetic socket modifications on physical function and patient-reported outcomes.Trials. 2022 Apr 12;23(1):299. doi: 10.1186/s13063-022-06205-z. Trials. 2022. PMID: 35413866 Free PMC article.
-
Factors Associated With Prolonged Length of Stay and Failed Lower Limb Prosthetic Fitting During Inpatient Rehabilitation.Arch Rehabil Res Clin Transl. 2020 Sep 19;2(4):100084. doi: 10.1016/j.arrct.2020.100084. eCollection 2020 Dec. Arch Rehabil Res Clin Transl. 2020. PMID: 33543107 Free PMC article.
References
-
- Landry GJ, Silverman DA, Liem TK, Mitchell EL, Moneta GL. Predictors of healing and functional outcome following transmetatarsal amputations. Arch Surg 2011;146:1005–9. - PubMed
-
- Cruz CP, Eidt JF, Capps C, Kirtley L, Moursi MM. Major lower extremity amputations at a Veterans Affairs hospital. Am J Surg 2003;186:449–54. - PubMed
-
- Dillingham TR, Pezzin LE, Shore AD. Reamputation, mortality, and health care costs among persons with dysvascular lower-limb amputations. Arch Phys Med Rehabil 2005;86: 480–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
