

Trends in Incidence of Hospitalized Acute Myocardial Infarction in the Cardiovascular Research Network (CVRN)
- PMID: 27751900
- PMCID: PMC5318252
- DOI: 10.1016/j.amjmed.2016.09.014
Trends in Incidence of Hospitalized Acute Myocardial Infarction in the Cardiovascular Research Network (CVRN)
Abstract
Background: Monitoring trends in cardiovascular events can provide key insights into the effectiveness of prevention efforts. Leveraging data from electronic health records provides a unique opportunity to examine contemporary, community-based trends in acute myocardial infarction hospitalizations.
Methods: We examined trends in hospitalized acute myocardial infarction incidence among adults aged ≥25 years in 13 US health plans in the Cardiovascular Research Network. The first hospitalization per member for acute myocardial infarction overall and for ST-segment elevation myocardial infarction and non-ST-segment elevation myocardial infarction was identified by International Classification of Diseases, Ninth Revision, Clinical Modification primary discharge codes in each calendar year from 2000 through 2008. Age- and sex-adjusted incidence was calculated per 100,000 person-years using direct adjustment with 2000 US census data.
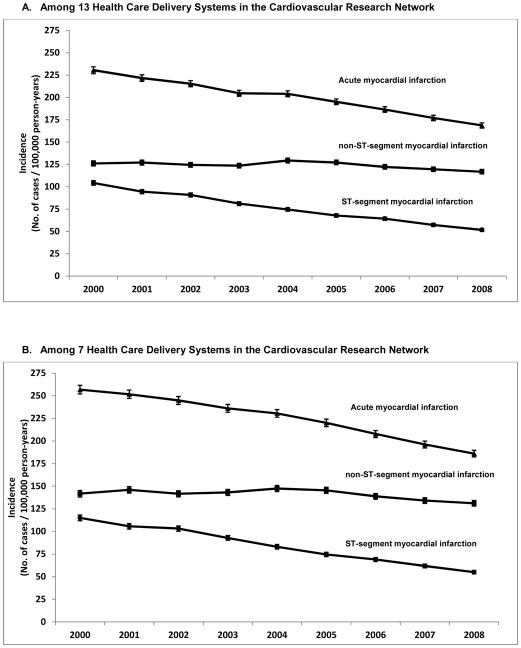
Results: Between 2000 and 2008, we identified 125,435 acute myocardial infarction hospitalizations. Age- and sex-adjusted incidence rates (per 100,000 person-years) of acute myocardial infarction decreased an average 3.8%/y from 230.5 in 2000 to 168.6 in 2008. Incidence of ST-segment elevation myocardial infarction decreased 8.7%/y from 104.3 in 2000 to 51.7 in 2008, whereas incidence of non-ST-segment elevation myocardial infarction increased from 126.1 to 129.4 between 2000 and 2004 and then decreased thereafter to 116.8 in 2008. Age- and sex-specific incidence rates generally reflected similar patterns, with relatively larger decreases in ST-segment elevation myocardial infarction rates in women compared with men. As compared with 2000, the age-adjusted incidence of ST-segment elevation myocardial infarction in 2008 was 48% lower among men and 61% lower among women.
Conclusions and relevance: Among a large, diverse, multicenter community-based insured population, there were significant decreases in incidence of hospitalized acute myocardial infarction and the more serious ST-segment elevation myocardial infarctions between 2000 and 2008. Decreases in ST-segment elevation myocardial infarctions were most pronounced among women. While ecologic in nature, these secular decreases likely reflect, at least in part, results of improvement in primary prevention efforts.
Keywords: Acute myocardial infarction; Cardiovascular disease; Epidemiology; Sex differences; Trends.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures
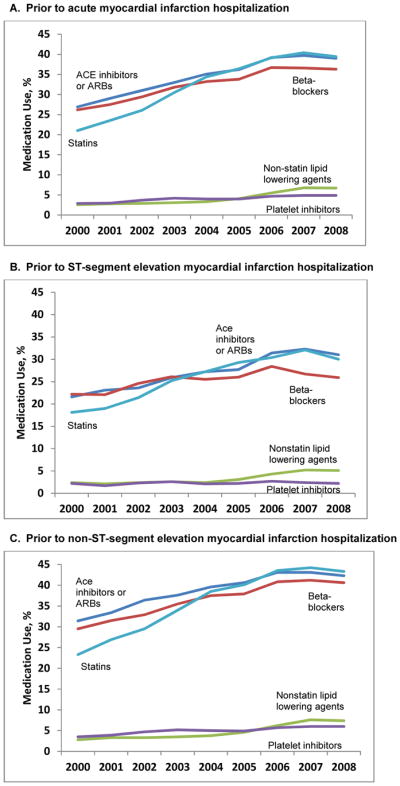
 bars represent 95% confidence intervals.
bars represent 95% confidence intervals.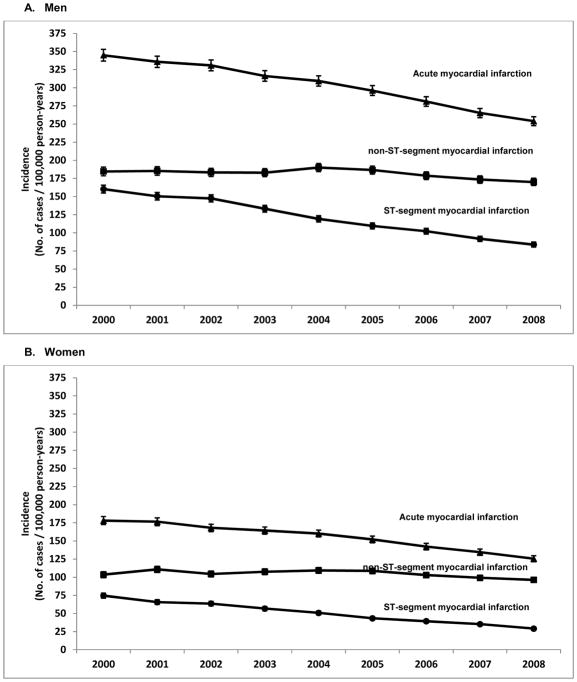 bars represent 95% confidence intervals.
bars represent 95% confidence intervals.References
-
- Mozaffarian D, Benjamin EJ, Go AS, et al. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation. 2015 - PubMed
-
- Sidney S, Rosamond WD, Howard VJ, Luepker RV National Forum for Heart Disease Stroke Prevention. The “heart disease and stroke statistics--2013 update” and the need for a national cardiovascular surveillance system. Circulation. 2013;127(1):21–23. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
