Vasopressor requirement during targeted temperature management for out-of-hospital cardiac arrest caused by acute myocardial infarction without cardiogenic shock
- PMID: 27752611
- PMCID: PMC5051625
- DOI: 10.15441/ceem.15.090
Vasopressor requirement during targeted temperature management for out-of-hospital cardiac arrest caused by acute myocardial infarction without cardiogenic shock
Abstract
Objective: We investigated whether patients with out-of-hospital cardiac arrest (OHCA) due to an acute myocardial infarction without cardiogenic shock required higher doses of vasopressors with low targeted temperature management (TTM) after return of spontaneous circulation.
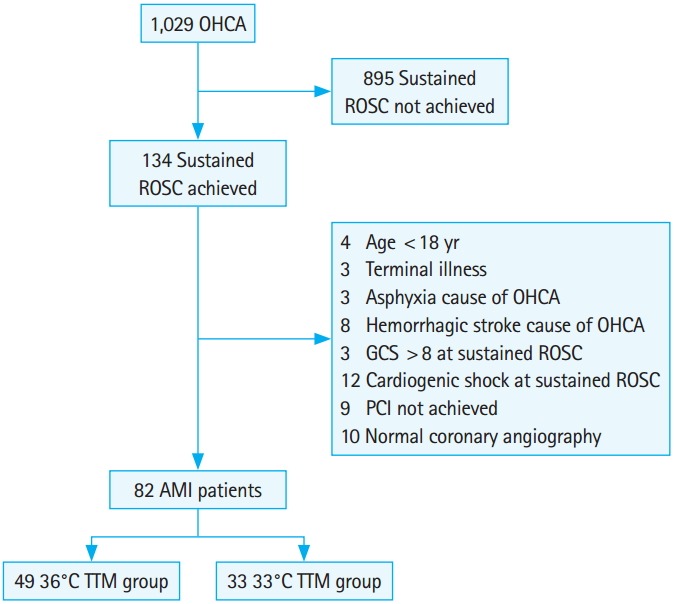
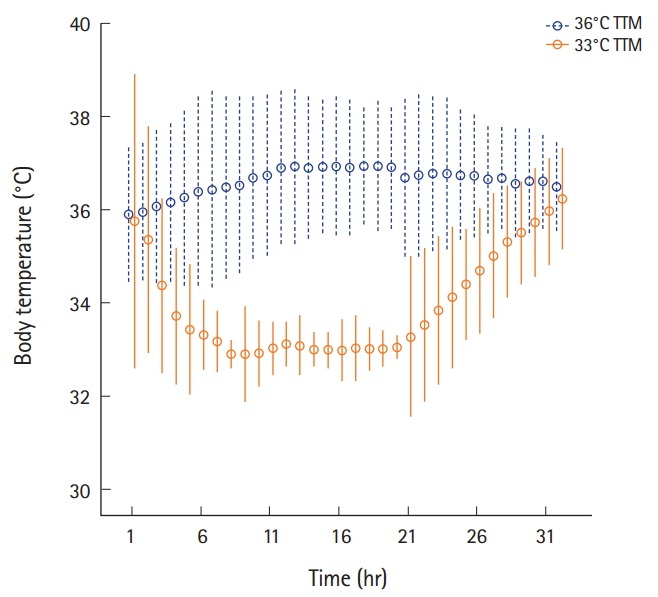
Methods: We included consecutive comatose patients resuscitated from OHCA between January 2011 and December 2013. Patients with return of spontaneous circulation, regional wall motion abnormality on echocardiography, and coronary artery stenosis of ≥70% on percutaneous coronary artery angiography were enrolled. These patients received 36°C TTM or 33°C TTM following approval of TTM by patients' next-of-kin (36°C and 33°C TTM groups, respectively). The cumulative vasopressor index was compared between groups.
Results: During induction phase, dose of vasopressors did not differ between groups. In the maintenance phase, the norepinephrine dose was 0.37±0.57 and 0.26±0.91 µg·kg-1·min-1 in the 33°C and 36°C TTM groups, respectively (P<0.01). During the rewarming phase, the norepinephrine and dopamine doses were 0.49±0.60 and 9.67±9.60 mcg·kg-1·min-1 in the 33°C TTM group and 0.14±0.46 and 3.13±7.19 mcg·kg-1·min-1 in the 36°C TTM group, respectively (P<0.01). The median cumulative vasopressor index was 8 (interquartile range, 3 to 8) and 4 (interquartile range, 0 to 8) in the 33°C and 36°C TTM groups, respectively (P=0.03).
Conclusion: In this study, patients with OHCA due to acute myocardial infarction without cardiogenic shock had an elevated vasopressor requirement with 33°C TTM compared to 36°C TTM during the maintenance and rewarming phases.
Keywords: Hypothermia; Myocardial infarction; Vasoconstrictor agents.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures

References
-
- Zipes DP, Wellens HJ. Sudden cardiac death. Circulation. 1998;98:2334–51. - PubMed
-
- Dekker LR, Bezzina CR, Henriques JP, et al. Familial sudden death is an important risk factor for primary ventricular fibrillation: a case-control study in acute myocardial infarction patients. Circulation. 2006;114:1140–5. - PubMed
-
- Reichenbach DD, Moss NS, Meyer E. Pathology of the heart in sudden cardiac death. Am J Cardiol. 1977;39:865–72. - PubMed
-
- Peberdy MA, Callaway CW, Neumar RW, et al. Part 9: postcardiac arrest care. 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;122(18 Suppl 3):S768–86. - PubMed
-
- Nolan JP, Neumar RW, Adrie C, et al. Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. A Scientific Statement from the International Liaison Committee on Resuscitation; the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; the Council on Stroke. Resuscitation. 2008;79:350–79. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous