

Impact of Operational Theater on Combat and Noncombat Trauma-Related Infections
- PMID: 27753561
- PMCID: PMC5123796
- DOI: 10.7205/MILMED-D-15-00368
Impact of Operational Theater on Combat and Noncombat Trauma-Related Infections
Abstract
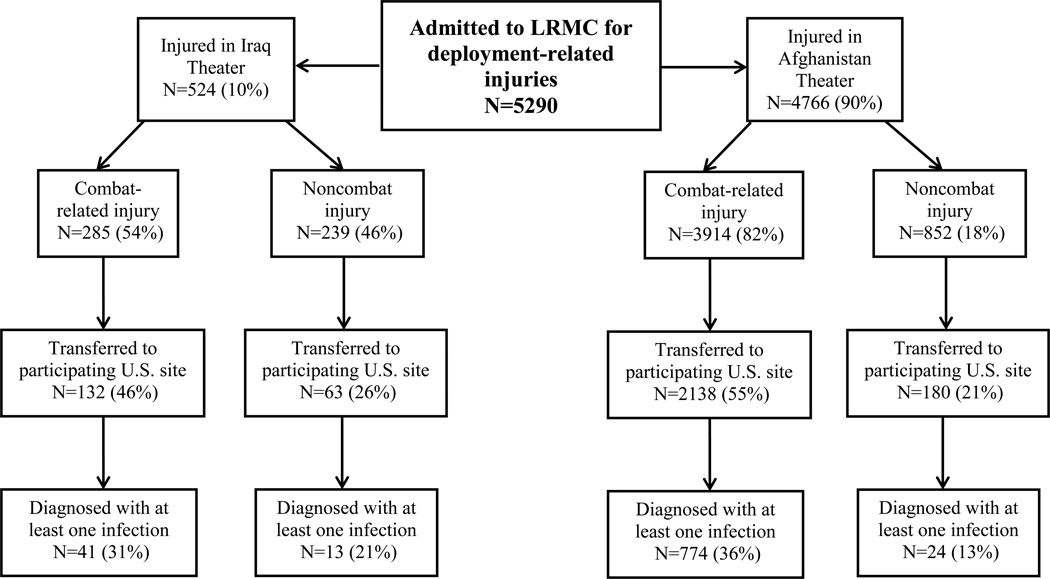
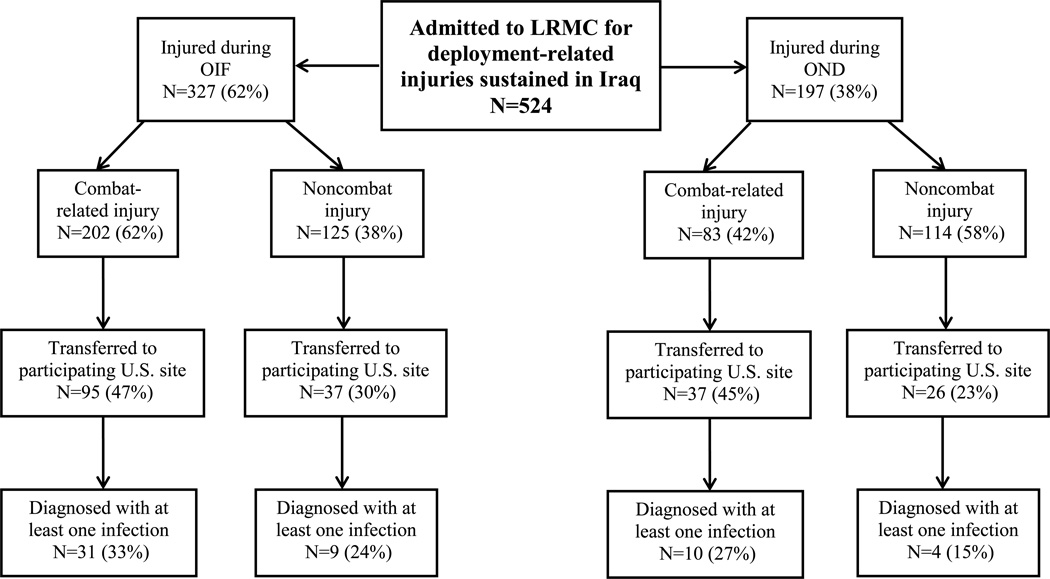
The Trauma Infectious Disease Outcomes Study began in June 2009 as combat operations were decreasing in Iraq and increasing in Afghanistan. Our analysis examines the rate of infections of wounded U.S. military personnel from operational theaters in Iraq and Afghanistan admitted to Landstuhl Regional Medical Center between June 2009 and December 2013 and transferred to a participating U.S. hospital. Infection risk factors were examined in a multivariate logistic regression analysis (expressed as odds ratios [OR]; 95% confidence intervals [CI]). The study population includes 524 wounded military personnel from Iraq and 4,766 from Afghanistan. The proportion of patients with at least one infection was 28% and 34% from the Iraq and Afghanistan theaters, respectively. The incidence density rate was 2.0 (per 100 person-days) for Iraq and 2.7 infections for Afghanistan. Independent risk factors included large-volume blood product transfusions (OR: 10.68; CI: 6.73-16.95), high Injury Severity Score (OR: 2.48; CI: 1.81-3.41), and improvised explosive device injury mechanism (OR: 1.84; CI: 1.35-2.49). Operational theater (OR: 1.32; CI: 0.87-1.99) was not a risk factor. The difference in infection rates between operational theaters is primarily a result of increased injury severity in Afghanistan from a higher proportion of blast-related trauma during the study period.
Reprint & Copyright © 2016 Association of Military Surgeons of the U.S.
Figures
References
-
- Murray CK, Hinkle MK, Yun HC. History of infections associated with combat-related injuries. J Trauma. 2008;64(3 Suppl):S221–S231. - PubMed
-
- Murray CK. Epidemiology of infections associated with combat-related injuries in Iraq and Afghanistan. J Trauma. 2008;64(3 Suppl):S232–S238. - PubMed
-
- Aronson NE, Sanders JW, Moran KA. In harm's way: infections in deployed American military forces. Clin Infect Dis. 2006;43(8):1045–1051. - PubMed
-
- Hospenthal DR, Murray CK, Andersen RC, Bell RB, Calhoun JH, Cancio LC, et al. Guidelines for the prevention of infections associated with combat-related injuries: 2011 update: endorsed by the Infectious Diseases Society of America and the Surgical Infection Society. J Trauma. 2011;71(2 Suppl 2):S210–S234. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
